Psoriasis is a chronic inflammatory skin disease characterized by well-defined erythematous plaques covered with silvery-white scales. It affects extensor surfaces, scalp, nails and intertriginous areas. The disease has a genetic predisposition and can be triggered by infections, medications, stress and trauma. Pathogenesis involves activation of the immune system including T cells which secrete cytokines leading to abnormal keratinocyte proliferation. Presentations include plaque, guttate, pustular and erythrodermic subtypes. Management involves topical agents, phototherapy and systemic medications such as retinoids, methotrexate and biologics that target cytokines like TNF-α. Complications include psor
Rosacea is a chronic (long-term) disease
that affects the skin and sometimes the eyes. The disorder is characterized by
redness, pimples, and, in advanced stages, thickened skin. Rosacea usually
affects the face. Skin on other parts of the upper body is only rarely
involved.
Rosacea is a chronic (long-term) disease
that affects the skin and sometimes the eyes. The disorder is characterized by
redness, pimples, and, in advanced stages, thickened skin. Rosacea usually
affects the face. Skin on other parts of the upper body is only rarely
involved.
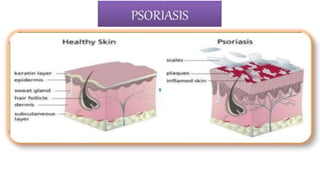
Psoriasis is a skin disease that causes red, itchy scaly patches, most commonly on the knees, elbows, trunk and scalp. Psoriasis is a common, long-term (chronic) disease with no cure. It tends to go through cycles, flaring for a few weeks or months, then subsiding for a while or going into remission
INTRODUCTION OF PSORIASIS, EPIDEMIOLOGY OF PSORIASIS, CLINICAL FEATURES OF PSORIASIS, PROGNOSIS OF PSORIASIS, HISTOPATHOLOGY OF PSORIASIS, TRIGGERING FACTORS OF PSORIASIS, PATHOGENESIS OF PSORIASIS
Introduction
Classification of the disease
History of disease
Epidemiology of disease
Clinical signs and symptoms
Genetic,
immunology and Pathogenesis
Diagnosis
Treatment
Vaccination
Prevention
Dermatitis, also known as eczema, is a group of diseases that results in inflammation of the skin. These diseases are characterized by itchiness, red skin and a rash. In cases of short duration, there may be small blisters
Psoriasis is a skin disease that causes red, itchy scaly patches, most commonly on the knees, elbows, trunk and scalp. Psoriasis is a common, long-term (chronic) disease with no cure. It tends to go through cycles, flaring for a few weeks or months, then subsiding for a while or going into remission
INTRODUCTION OF PSORIASIS, EPIDEMIOLOGY OF PSORIASIS, CLINICAL FEATURES OF PSORIASIS, PROGNOSIS OF PSORIASIS, HISTOPATHOLOGY OF PSORIASIS, TRIGGERING FACTORS OF PSORIASIS, PATHOGENESIS OF PSORIASIS
Introduction
Classification of the disease
History of disease
Epidemiology of disease
Clinical signs and symptoms
Genetic,
immunology and Pathogenesis
Diagnosis
Treatment
Vaccination
Prevention
Dermatitis, also known as eczema, is a group of diseases that results in inflammation of the skin. These diseases are characterized by itchiness, red skin and a rash. In cases of short duration, there may be small blisters
Know more about Psoriasis ,Types and TreatmentsiCliniq
Psoriasis is a prototypic papulosquamous skin
diseases characterised by erythematous papules. It is a chronic inflammatory skin disease with increased epidermal proliferation related to dysregulation of the immune system.
It needs long time medication to get it control, the permanent is not found yet.
To Get guidance to treat Psoriasis from a doctor --> https://www.icliniq.com/ask-a-doctor-online/dermatologist/psoriasis
Know all about psoriasis, its types and treatment options both with allopathic and homeopathic systems of medicines. we detail about the complete aetiology, causes, types, illustrated with pictures, and the allopathic and homeopathic modes of treatment . here we explain how homeopathy helps in controlling and making the skin better in psoriasis and the complete treatment protocols and time required to see favourable results.
Acetabularia Information For Class 9 .docxvaibhavrinwa19
Acetabularia acetabulum is a single-celled green alga that in its vegetative state is morphologically differentiated into a basal rhizoid and an axially elongated stalk, which bears whorls of branching hairs. The single diploid nucleus resides in the rhizoid.
The Roman Empire A Historical Colossus.pdfkaushalkr1407
The Roman Empire, a vast and enduring power, stands as one of history's most remarkable civilizations, leaving an indelible imprint on the world. It emerged from the Roman Republic, transitioning into an imperial powerhouse under the leadership of Augustus Caesar in 27 BCE. This transformation marked the beginning of an era defined by unprecedented territorial expansion, architectural marvels, and profound cultural influence.
The empire's roots lie in the city of Rome, founded, according to legend, by Romulus in 753 BCE. Over centuries, Rome evolved from a small settlement to a formidable republic, characterized by a complex political system with elected officials and checks on power. However, internal strife, class conflicts, and military ambitions paved the way for the end of the Republic. Julius Caesar’s dictatorship and subsequent assassination in 44 BCE created a power vacuum, leading to a civil war. Octavian, later Augustus, emerged victorious, heralding the Roman Empire’s birth.
Under Augustus, the empire experienced the Pax Romana, a 200-year period of relative peace and stability. Augustus reformed the military, established efficient administrative systems, and initiated grand construction projects. The empire's borders expanded, encompassing territories from Britain to Egypt and from Spain to the Euphrates. Roman legions, renowned for their discipline and engineering prowess, secured and maintained these vast territories, building roads, fortifications, and cities that facilitated control and integration.
The Roman Empire’s society was hierarchical, with a rigid class system. At the top were the patricians, wealthy elites who held significant political power. Below them were the plebeians, free citizens with limited political influence, and the vast numbers of slaves who formed the backbone of the economy. The family unit was central, governed by the paterfamilias, the male head who held absolute authority.
Culturally, the Romans were eclectic, absorbing and adapting elements from the civilizations they encountered, particularly the Greeks. Roman art, literature, and philosophy reflected this synthesis, creating a rich cultural tapestry. Latin, the Roman language, became the lingua franca of the Western world, influencing numerous modern languages.
Roman architecture and engineering achievements were monumental. They perfected the arch, vault, and dome, constructing enduring structures like the Colosseum, Pantheon, and aqueducts. These engineering marvels not only showcased Roman ingenuity but also served practical purposes, from public entertainment to water supply.
Unit 8 - Information and Communication Technology (Paper I).pdfThiyagu K
This slides describes the basic concepts of ICT, basics of Email, Emerging Technology and Digital Initiatives in Education. This presentations aligns with the UGC Paper I syllabus.
Synthetic Fiber Construction in lab .pptxPavel ( NSTU)
Synthetic fiber production is a fascinating and complex field that blends chemistry, engineering, and environmental science. By understanding these aspects, students can gain a comprehensive view of synthetic fiber production, its impact on society and the environment, and the potential for future innovations. Synthetic fibers play a crucial role in modern society, impacting various aspects of daily life, industry, and the environment. ynthetic fibers are integral to modern life, offering a range of benefits from cost-effectiveness and versatility to innovative applications and performance characteristics. While they pose environmental challenges, ongoing research and development aim to create more sustainable and eco-friendly alternatives. Understanding the importance of synthetic fibers helps in appreciating their role in the economy, industry, and daily life, while also emphasizing the need for sustainable practices and innovation.
2024.06.01 Introducing a competency framework for languag learning materials ...Sandy Millin
http://sandymillin.wordpress.com/iateflwebinar2024
Published classroom materials form the basis of syllabuses, drive teacher professional development, and have a potentially huge influence on learners, teachers and education systems. All teachers also create their own materials, whether a few sentences on a blackboard, a highly-structured fully-realised online course, or anything in between. Despite this, the knowledge and skills needed to create effective language learning materials are rarely part of teacher training, and are mostly learnt by trial and error.
Knowledge and skills frameworks, generally called competency frameworks, for ELT teachers, trainers and managers have existed for a few years now. However, until I created one for my MA dissertation, there wasn’t one drawing together what we need to know and do to be able to effectively produce language learning materials.
This webinar will introduce you to my framework, highlighting the key competencies I identified from my research. It will also show how anybody involved in language teaching (any language, not just English!), teacher training, managing schools or developing language learning materials can benefit from using the framework.
A Strategic Approach: GenAI in EducationPeter Windle
Artificial Intelligence (AI) technologies such as Generative AI, Image Generators and Large Language Models have had a dramatic impact on teaching, learning and assessment over the past 18 months. The most immediate threat AI posed was to Academic Integrity with Higher Education Institutes (HEIs) focusing their efforts on combating the use of GenAI in assessment. Guidelines were developed for staff and students, policies put in place too. Innovative educators have forged paths in the use of Generative AI for teaching, learning and assessments leading to pockets of transformation springing up across HEIs, often with little or no top-down guidance, support or direction.
This Gasta posits a strategic approach to integrating AI into HEIs to prepare staff, students and the curriculum for an evolving world and workplace. We will highlight the advantages of working with these technologies beyond the realm of teaching, learning and assessment by considering prompt engineering skills, industry impact, curriculum changes, and the need for staff upskilling. In contrast, not engaging strategically with Generative AI poses risks, including falling behind peers, missed opportunities and failing to ensure our graduates remain employable. The rapid evolution of AI technologies necessitates a proactive and strategic approach if we are to remain relevant.
Honest Reviews of Tim Han LMA Course Program.pptxtimhan337
Personal development courses are widely available today, with each one promising life-changing outcomes. Tim Han’s Life Mastery Achievers (LMA) Course has drawn a lot of interest. In addition to offering my frank assessment of Success Insider’s LMA Course, this piece examines the course’s effects via a variety of Tim Han LMA course reviews and Success Insider comments.
Read| The latest issue of The Challenger is here! We are thrilled to announce that our school paper has qualified for the NATIONAL SCHOOLS PRESS CONFERENCE (NSPC) 2024. Thank you for your unwavering support and trust. Dive into the stories that made us stand out!
Biological screening of herbal drugs: Introduction and Need for
Phyto-Pharmacological Screening, New Strategies for evaluating
Natural Products, In vitro evaluation techniques for Antioxidants, Antimicrobial and Anticancer drugs. In vivo evaluation techniques
for Anti-inflammatory, Antiulcer, Anticancer, Wound healing, Antidiabetic, Hepatoprotective, Cardio protective, Diuretics and
Antifertility, Toxicity studies as per OECD guidelines
Francesca Gottschalk - How can education support child empowerment.pptxEduSkills OECD
Francesca Gottschalk from the OECD’s Centre for Educational Research and Innovation presents at the Ask an Expert Webinar: How can education support child empowerment?
Francesca Gottschalk - How can education support child empowerment.pptx
Psoriasis
1.
2. Introduction of Psoriasis
Psoriasis is a chronic inflammatory, hyperproliferative skin disease. It is
characterized by well-defined, erythematous plaque with silvery-white surface
scale. Distribution includes extensor surfaces (i.e., knees, elbows, and buttocks)
In about 25% of cases, peculiar pitting of nails is seen. Psoriatic arthritis
resembling rheumatoid arthritis is produced in about 5% of cases but
rheumatoid factor is absent. may also involve palms and scalp (particularly
anterior scalp margin). Associated findings include psoriatic arthritis and nail
changes (onycholysis, pitting or thickening of nail plate with accumulation of
subungual debris).
3. History of Psoriasis
The word psoriasis is derived from Greek word ‘psora’ means itching.
The Greek physician Galen of perganon (130-200 BC) use the term
Psoriasis vulgaris to refer all dermo and epidermopathies accompanied by
pruiritis.
Since 1950 local application and systemic medications are used for the
psoriasis.
4. EPIDEMIOLOGY
Psoriasis is the most commonly recognized papulosquamous disease. It occurs in 2 to 3% of the
general population, with considerable variation in different parts of the world.
Lower rates are found in Japanese and psoriasis is rare in West Africans.
It affects male and female patients equally.
Approximately one third of the patients have a positive family history.
Psoriasis has a bimodal peak of onset, at age 22.5 years and again at age 55 years.
The onset of psoriasis before the age of 15 years is associated with a higher prevalence of
positive family history of psoriasis and with more severe disease.
Recent epidemiologic studies have shown that psoriasis is associated with an increased risk of
heart attack and strokes, a relationship that may be related to a chronic inflammatory state.
Psoriasis is also associated in up to 10% of patients with arthritis, which in some cases may be
severe.
5. PATHOBIOLOGY
Psoriasis involves the innate and adaptive immune systems, with abnormal
keratinocyte proliferation. Factors playing a role in the pathogenesis include
activation of antigen-presenting cells and development of TH1 and TH17
cells. Mediators include interleukin-12 (IL-12), IL-23, tumor necrosis factor-α
(TNF-α), and interferon-γ.
Exposure to precipitating factors such as infections (e.g., streptococcal or HIV
infections), stress, or physical injury results in activation of T cells and
generation of cytokines, followed by influx of neutrophils and subsequent
release of inflammatory mediators, which lead to the development of
cutaneous lesions.
Psoriasis has a complex, polygenetic inheritance. Susceptibility genes include
PSORS1 to PSORS9, although PSORS1, mapped to chromosome 6p21.3, is
now considered a major locus for susceptibility to psoriasis.
6. Psoriasis is a multifactorial immunologic disease, both genetic (e.g., human
leukocyte antigen [HLA] types) and environmental factors contribute to risk.
It is not known if the inciting antigens are self or environmental. Sensitized
populations of T cells home to the dermis, including CD4+ TH17 and TH1
cells and CD8+ T cells, and accumulate in the epidermis.
These cells secrete cytokines and growth factors that induce keratinocyte
hyperproliferation, resulting in the characteristic lesions.
Psoriatic lesions can be induced in susceptible persons by local trauma
(Koebner phenomenon), which may induce a local inflammatory response
that promotes lesion development.
GWAS studies have linked an increased risk of psoriasis to polymorphisms in
HLA loci and genes affecting antigen presentation, TNF signaling, and skin
barrier function.
PATHOGENESIS
8. SILVER SCALING OF SKIN
LARGE PRODUCTION OF VARIOUS CYTOKINES ( INTEFERRON,
INTERLEUKIN-12)
SUPERFICIAL BLOOD VESSEL DILATED AND VASCULAR ENGORGEMENT
EPIDERMAL HYPERPLASIA AND IMPROPER CELL MATURATION
FAILS TO RELEASE ADEQUATE LIPIDS WHICH LEAD TO FLAKING,
SCALING PRESENTATION OF PSORIASIS LESION
Cont…
9. Etiology of Psoriasis
(1)Unknown
(2)Genetic
Some factor may aggravated the condition such as:-
Trauma
• Psoriatic lesions can appear at sites of skin trauma, such as scratches or surgical wounds (Kobner
isomorphic phenomenon)
Infection
• β-hemolytic streptococcal throat infections often precede guttate psoriasis.
• Severe psoriasis may be the initial presentation of HIV infection.
Sunlight
• sun exposure, mainly due to Kobnerisation at sites of sunburn or polymorphic light eruption.
Drugs
• Antimalarials, β-adrenoceptor antagonists (β-blockers), lithium, NSAIDs and anti-TNF-α drugs.
Psychological factors
• Anxiety and stress may exacerbate psoriasis.
Smoking and Alcohol
Obesity
Hormonal changes
10. Types of Psoriasis
1) Plaque psoriasis
2) Guttate psoriasis
3) Inverse psoriasis
4) Pustular psoriasis
• Localised
• Grneralised
5) Local forms of psoriasis
• Palmoplanter
• Scalp
• Nail (psoriatic onychodystrophy)
6) Psoriatic arthritis
11.
12. Plaque Psoriasis
Most common type affects
approximately 85%.
Features pink, well defined
plaques with silver scale.
Lesion may be single or
numerous.
Plaque may involve large areas
of skin.
Classically affects elbows,
Knees, buttocks and scalp.
13. Guttate psoriasis
Guttate psoriasis usually occurs after viral or
bacterial (most commonly streptococcal)
infection.
This is most common in children and
adolescents.
It is commonly associated with HLA Cw6.
Individual lesions are droplet-shaped, small
(usually less than 1 cm in diameter),
erythematous, scaly and numerous.
An episode of guttate psoriasis may clear
spontaneously or with topical treatment within
a few months, but UVB phototherapy is often
required and is highly effective.
Guttate psoriasis often heralds the onset of
plaque psoriasis in adulthood.
14. Inverse or flexural
psoriasis
psoriasis that occurs in skinfold
areas such as the groin, axilla,
and inframammary folds.
It appears as an erythematous,
somewhat shiny patch because
of the constant friction in the
involved areas, scales are
usually absent.
May cause diagnostic difficulty
when genital or perianal region
is affected in isolation.
15. Generalized pustular psoriasis is uncommon, unstable and life-threatening. It
will often emerge in the context of plaque disease and the onset is usually
sudden, with large numbers of small sterile pustules on aerythematous
background, often merging into sheets, with waves of new pustules in
subsequent days.
The patient is usually febrile and systemically unwell, and this must be dealt
with as a medical emergency.
Pustular psoriasis
Pustular psoriasis may be generalized or localized.
Localised pustular psoriasis of the palms and soles (palmoplantar pustulosis) is
more common, chronic and closely associated with smoking; small, sterile
pustules and erythema develop and resolve with pigmentation and scaling.
A localised form of sterile pustulosis of a few digits (acropustulosis) can also
occur.
It is unclear whether these localised forms of pustulosis are truly psoriatic.
16. Erythrodermic psoriasis
Generalized erythema covering entire
skin surface.
May evolve slowly from chronic plaque
psoriasis or appear as eruptive
phenomenon.
Patients may become febrile,
hypo/hyperthermic and dehydrated.
Complication include cardiac failure,
infections, malabsorption and anemia.
Relatively uncommon
17. Palmoplantar psoriasis
Can be hyperkeratotic or pustular.
May mimic dermatitis look for
psoriatic manifestations elsewhere to
aid diagnosis.
Possibly aggravated by trauma.
18. Scalp psoriasis
Varies from minor scaling with
erythema to thick hyperkeratotic
plaques.
May extend beyond hairline.
Patient scratching may produce
asymmetric plaques.
19. Nail psoriasis
May be present in patients with any type of
psoriasis.
Can take several forms:-
Pitting:- Discrete, well circumscribed
depressions on nail surface.
Subungual hyperkeratosis:- Silvery white
crusting under free edge of nail with some
thickening of nail plate.
Onycholysis:- Nail separates from nail bed
at free edge.
Oil drop sign:- Pink/red colour change on
nail surface.
20. Psoriatic Arthritis
Five to 30% of patients with psoriasis
may also have psoriatic arthritis,
which may precede the appearance of
cutaneous lesions 95% of these
patients present with peripheral
asymmetrical oligoarthritis involving
the interphalangeal joints of the hands
and feet, while 5% have exclusively
axial or skeletal disease.
Psoriatic arthritis has been associated
with HLAB57, although some studies
have also reported HLA-Cw6 in more
than 50% of all persons with this
disease.
21. It will vary according to types of at psoriasis. Initially the first sign of
psoriasis is often red spots on the body.
The patches of skin
Dry, swollen and inflammed Covered with silver white flakes Raised and
thick skin.
Other symptoms of psoriasis includes:- Pain, itching and burning.
Restricted joint motion or pain Cracked and bleeding skin.
Dandruff on scalp
Pus filled blisters Genital lesions in males.
Pitting, small depression on the surface of the nail Yellow, dicsolored nail
Koebner phenomenon
Arthriti
COMMON CLINICAL MANIFESTATIONS
22.
23. 1)Auspitzsign(Grattage test):- Removing
the scale reveals a smooth, red, glossy
membrane with tiny punctate bleeding
point.
2) Rich red color:- often referred to as
'salmon pink‘. This quality of color is of
special diagnostic value to differentiate
psoriasis from eczema in lesions on the
palms, soles and scalp.
3) Candle grease sign
4) Koebner’s or Isomorphic phenomenon
5) Holo or Woronoff sign
Signs of psoriasis
24. PASI Score (Psoriasis Area and Severity Index)
■It is a method to estimate severity of psoriasis in order to evaluate the clinical
efficacy of new treatments
■Psoriatic plaques are graded based on three criteria: redness (R), thickness (T),
and scaliness (S)
■Severity is rated on a 0-4 scale (0 for no involvement up to 4 for severe
involvement)
■The highest PASI score is 12; the lowest is 0
25.
26. Diagnostic Investigations
Collect history
Physical examinations
Skin biopsy :- under local anesthesia
Blood and radiography test was done to rule out psoriatic arthritis
TLC ,ESR, C- Reactive protein, Serum calcium, Serum uric acid.
Immunoglobulin
Anti-nuclear antibody
Nail dipping and skin scraping
Throat swab
28. Complications
Infection
Fluid and electrolyte imbalance
Low self esteem
Depression
Stress
Metabolic syndrome (increased blood pressure, high blood sugar, excess
body fat around the waist, and abnormal cholesterol levels)
Hypertension
Joint damage
29. Management of psoriasis
Therapy includes
1) Topical medications
2) UV-based treatment
3) Systemic drugs
For mild disease, topical therapy with topical corticosteroids(e.g.,
triamcinolone ointment, 0.1% twice daily for 1 to 2 weeks).
Calcipotriene cream (0.005%, twice daily as needed).
Tazarotene gel (0.05%, once or twice daily as needed), used alone or in
combination, is effective.
30. UV-based treatment
In patients who have widespread lesions, NB-UVB isthe best option, whereas
PUVA should be considered for patients in whom NB-UVB therapy has failed.
Systemic drugs
For patients with recalcitrant disease, oral medications such as
Methotrexate (7.5 to 15 mg/week)
Acitretin (25 to 50 mg/day)
Cyclosporine (3 to 5 mg/kg/day)
Hydroxyurea (1 g/day)
Mycophenolate mofetil (1 to 2 g/day) have all been used with success.
31. Topical agents Photo(chemo)
therapies
Systemic agents Intensive inpatient or
day-patient care
Emollients
tars
UVB Retinoids Topical agents and
photo(chemo)therapie
s under medical
supervision
dithranol
vitamin D
agonists,
PUVA Immunosuppressants, e.g.
methotrexate, ciclosporin,
mycophenolate,
hydroxycarbamide
retinoids, excimer laser Immunomodulators, e.g.
fumaric acid esters
corticosteroids Biological
immunosuppressants, e.g.
infliximab, etanercept,
adalimumab
Treatment categories in psoriasis
32. BIOLOGIC
AGENTS
DOSE/DURATION MONITORING SIDE EFFECTS
TNF-α
INHIBITORS
Etanercept
(Enbrel)
50 mg SC twice a week for 12 wk, then
50 mg SC weekly indefinitely
PPD CBC, LFT Injection site reaction,
infection
Infliximab
(Remicade)
5-10 mg/kg IV at weeks 0, 2, 6, then
every 8 wk indefinitely
PPD CBC, LFT Infusion reaction,
sepsis, lupus-like
syndrome, aplastic
anemia (rare)
Adalimumab
(Humira)
80 mg SC at week 0, 40 mg at wk 1,
then 40 mg every 2 wk indefinitely
PPD CBC, LFT Injection site reaction,
infection
ANTI-CD2
Alefacept (Amevive) 15 mg IM weekly for 12-16 wk; consider a
second course after a 12-wk interval
CD4 Infection
ANTI–IL-12/23
Ustekinumab (Stelara) SC at weeks 0, 4, then every 12 wk 100 kg: 90
mg indefinitely
PPD Infection
BIOLOGIC AGENTS FOR PSORIASIS