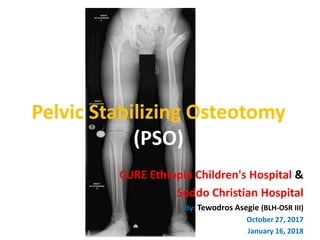
Pelvic stabilizing osteotomy (PSO) is a surgical procedure used to treat hip instability. It involves performing a valgus osteotomy of the proximal femur and sometimes a varus osteotomy of the distal femur. This realigns the hip to improve biomechanics and stability. For patient Abonesh, who has a dislocated left hip, previous girdlestone procedure, and limb length discrepancy, a PSO may be a suitable option to reduce pain, equalize limb length, and improve hip function and gait. Careful preoperative planning including measurement of adduction contracture and overcorrection angle is required to determine the degree of valgus angulation needed at the proximal osteotomy