Downloaded 145 times










![COMPARISON OF CYCLOOXYGENASE (COX-1& COX-2)
ENZYMES
Properties COX-1 COX-2
Site of action Found in many tissues, important for
homeostasis
Induced by inflammatory
stimuli at the site of
inflammation
Effects of activation Converts arachidonic acid to
inflammatory prostaglandins
Maintains renal function
Provides integrity to gastric mucosa
[cytoprotective].
Promotes vascular homeostasis
Autocrine effects cause fever
Increases pain, inflammation
Vasodilatory effects
Blocks platelet clumping
Effects of blocking Decreases swelling, pain and
inflammation.
Decreases pain and
inflammation
Effects of blocking
for a prolonged
period leads to
adverse effects like
Damage to renal system (acute
tubular necrosis may occur).
Sodium retention, edema, increased
blood pressure
Gastrointestinal erosions (ulcer) and
bleeding etc.
Decreases fever
Prevents protective
vasodilation, allows platelet
clumping, which can lead to
myocardial infarction,
cerebrovascular accidents. (on
prolonged use)](https://image.slidesharecdn.com/pgsnnsaids-190704054536/75/Prostaglandins-NSAIDS-13-2048.jpg)


















































![COMPARISON OF CYCLOOXYGENASE (COX-1& COX-2)
ENZYMES
Properties COX-1 COX-2
Site of action Found in many tissues, important for
homeostasis
Induced by inflammatory stimuli
at the site of inflammation
Effects of activation Converts arachidonic acid to
inflammatory prostaglandins
Maintains renal function
Provides integrity to gastric mucosa
[cytoprotective].
Promotes vascular homeostasis
Autocrine effects cause fever
Increases pain, inflammation
Vasodilatory effects
Blocks platelet clumping
Effects of blocking Decreases swelling, pain and
inflammation.
Decreases pain and
inflammation
Effects of blocking
for a prolonged
period leads to
adverse effects like
Damage to renal system (acute tubular
necrosis may occur).
Sodium retention, edema, increased
blood pressure
Gastrointestinal erosions (ulcer) and
bleeding etc.
Decreases fever
Prevents protective
vasodilation, allows platelet
clumping, which can lead to
myocardial infarction,
cerebrovascular accidents. (on
prolonged use)](https://image.slidesharecdn.com/pgsnnsaids-190704054536/75/Prostaglandins-NSAIDS-65-2048.jpg)

















































![EFFECTS OF NSAIDs
BENEFICIAL EFFECTS TOXIC EFFECTS
• Anti-inflammatory
• Antipyretic
• Analgesic effects
• Antithrombotic
• Closure of ductus arteriosus
in newborn
• GI ulcer
• Asthma precipitation
• Anaphylactic reaction in
susceptible individuals
• Rash & pruritus
• Sodium and water retention,
hyperkalemia, and
proteinuria.
• Delay/prolongation of labour
• Bleeding [Prolong bleeding
time]
• Abnormal liver function tests](https://image.slidesharecdn.com/pgsnnsaids-190704054536/75/Prostaglandins-NSAIDS-115-2048.jpg)
![NONSELECTIVE COX INHIBITORS (TRADITIONAL NSAIDs)
Groups Drug name t ½ [hours] Dose
Salicylates Aspirin 0.25-5
[dose
dependent]
• As Antiplatelet: 40-80 mg/day
• In Pain/fever: 325-650 mg QID
• In Rheumatic fever: 1 g every QID
• In Rheumatoid arthritis: 3-5 gm, OD
• As Antiinflammatory: 1.2-1.5 gm, TDS
• Children: 10 mg/kg every QID
• All above doses are oral.
Propionic acid
derivatives
Ibuprofen 2-4 400-600 mg TDS, oral
Naproxen 14 250mg BD/TDS, oral
Ketoprofen 1.8 50-100 mg BD/TDS, oral
Flurbiprofen 6 50 mg BD/QID, oral
Fenamate Mephenami
c acid
2-3 250-500 mg TDS, oral
Enolic acid
derivatives
Piroxicam 57 20 mg OD/BD, oral, 20mg/1 ml, i.m.
Acetic acid
derivatives
Ketorolac 4-6 10-20 mg QID, oral 30mg/1ml i.v./i.m.
Indomethac
in
2.5 25-50 mg BD/QID, oral
Nabumeton
e
24 500 mg OD, oral
Sulindac 7 150-200 mg BD, Oral
Pyrazolone
derivatives
Phenylbutazone, propiphenazone ,Oxyphenbutazone, Metamezol etc.](https://image.slidesharecdn.com/pgsnnsaids-190704054536/75/Prostaglandins-NSAIDS-116-2048.jpg)
![PREFERENTIAL COX-2 INHIBITORS
Drug name t ½ [hours] Dose
Nimesulide 2-5 100 mg BD, oral
Diclofenac 1-2 50 BD/TDS, oral
75 mg i.v./i.m., 1% topical gel
Aceclofenac - 100 mg BD, oral
Meloxicam 15-20 7.5-15 mg OD, oral
Piroxicam 45-50 20 mg/day OD, oral
Etodolac 7 200-400 mg BD/TDS, oral](https://image.slidesharecdn.com/pgsnnsaids-190704054536/75/Prostaglandins-NSAIDS-117-2048.jpg)
![SELECTIVE COX-2 INHIBITORS
Drug name t ½ [hours] Dose
Celecoxib 6-12 100-200 mg BD, oral
Etoricoxib 24 60-120 mg OD, oral
Parecoxib - 40 mg BD-QID, i.v.,i.m., oral
ANALGESIC-ANTIPYRETICS WITH POOR ANTIINFLAMMATORY ACTION
Groups Drug name t ½ [hours] Dose
Paraaminophenol
derivative
Paracetamol
(Acetaminophen)
2 500 mg QID, oral.
300mg/2ml i.m.
Pyrazolone derivatives Metamizol - 0.5–1.5 g oral/i.m./i.v.
Propiphenazone - 300–600 mg TDS.
Benzoxazocine
derivative
Nefopam 20-60 mg TDS
20mg i.m. QID](https://image.slidesharecdn.com/pgsnnsaids-190704054536/75/Prostaglandins-NSAIDS-118-2048.jpg)










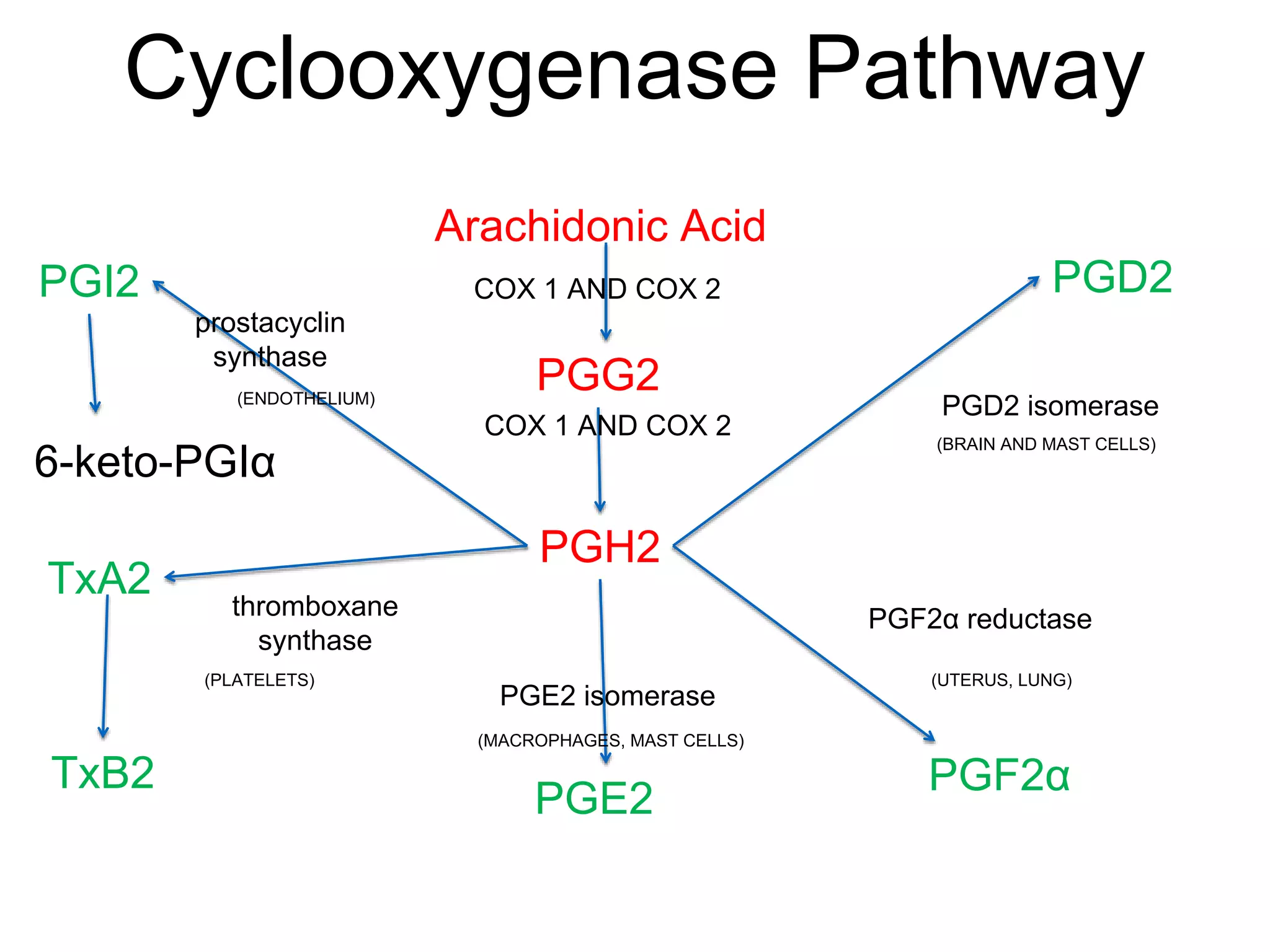
Prostaglandins are lipid compounds produced in the body from fatty acids. They have diverse functions and are involved in processes like inflammation, the menstrual cycle, pregnancy, and blood clotting. There are two main enzymes - COX-1 and COX-2 - that convert arachidonic acid into prostaglandins like PGE2, PGF2α, PGI2, and TXA2. These prostaglandins act through G-protein coupled receptors and have effects like smooth muscle contraction, vasodilation, and platelet aggregation. Nonsteroidal anti-inflammatory drugs (NSAIDs) work by inhibiting the COX enzymes and thereby reducing prostaglandin production, which is responsible























































































