Downloaded 135 times

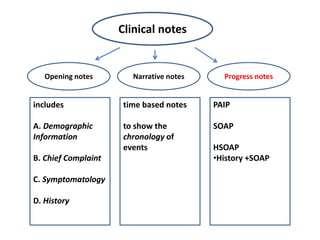


The document provides information on progress notes including: - Progress notes are used to document a patient's clinical status and progress over time during hospitalization or outpatient care. - They serve to communicate findings between healthcare professionals and allow retrospective review of a patient's case. - Progress notes are intended to be concise and provide communication about a patient's condition to those accessing their health record. Physicians and nurses are generally required to generate progress notes on a regular basis.









































































































