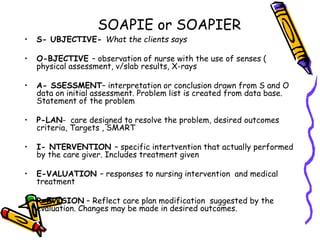
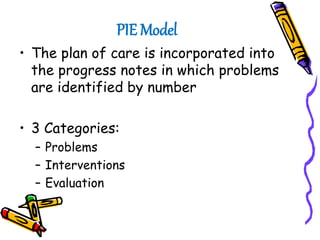
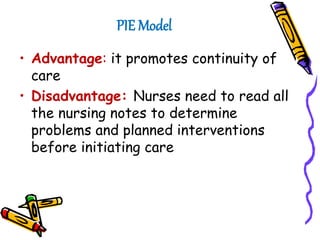
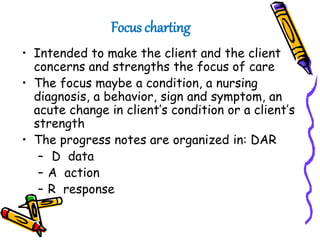
The document discusses guidelines for effective nursing documentation. It outlines content, timing, format, accountability, and confidentiality guidelines. It also discusses the purpose of client records for communication, planning care, auditing, research, education, reimbursement, and legal documentation. Finally, it describes different documentation systems like source-oriented records, problem-oriented records, nursing care plans, flow sheets, and computerized documentation.


![[1] documentation and reporting](https://cdn.slidesharecdn.com/ss_thumbnails/1documentationandreporting-150205213856-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)
















































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)

















