Downloaded 107 times
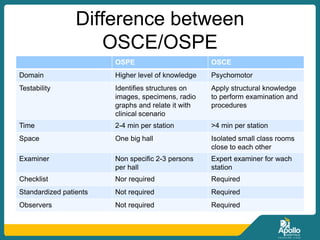
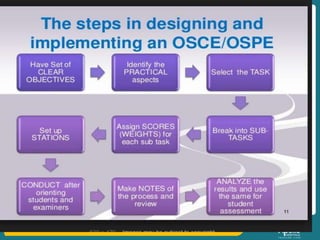
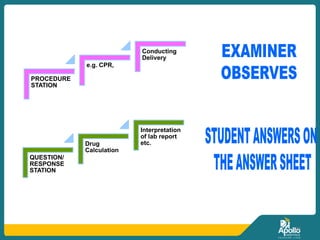



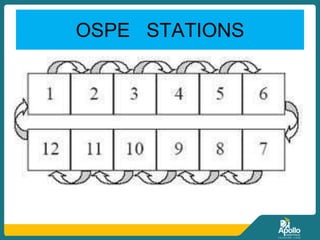
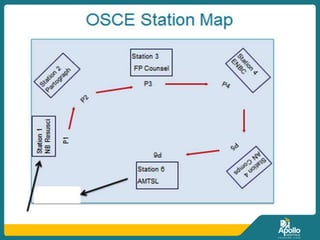

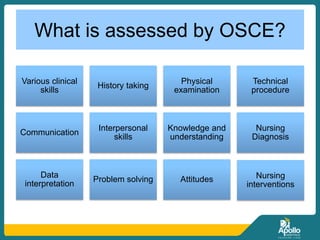
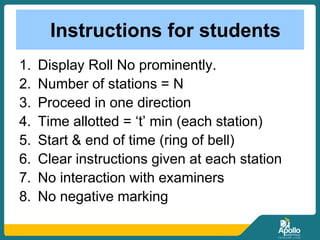
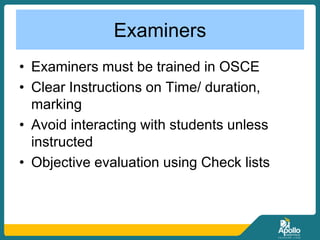
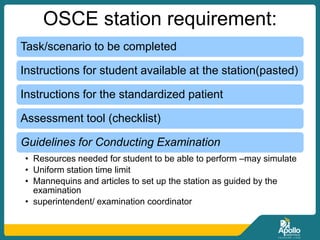




This document provides an overview of Objective Structured Clinical Examination (OSCE) and Objective Structured Practical Examination (OSPE). It discusses the background, purposes, methodology, advantages and disadvantages of OSCE/OSPE. Key points include that OSCE/OSPE aims to objectively and reliably evaluate clinical skills through structured stations using checklists. Stations typically last 3-10 minutes and assess skills like history taking, physical exams, procedures. OSCE/OSPE provides a standardized way to assess students and has been found to improve evaluation objectivity and student satisfaction compared to traditional exams. Challenges include the significant planning and resources required to implement OSCE/OSPE effectively.






















































































