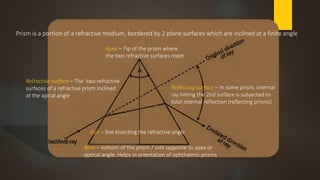
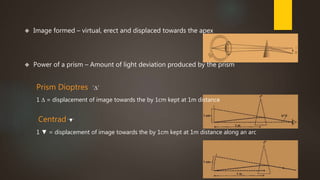
1. Prism is a portion of a refractive medium bounded by two plane surfaces inclined at an angle. It deviates light passing through it towards its base due to refraction.
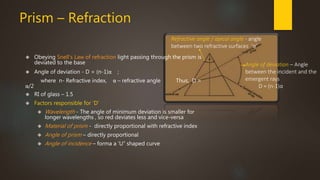
2. The angle of deviation (D) of a prism is determined by its refractive index (n) and refractive angle (α) using the formula D = (n-1)α.
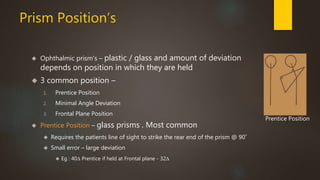
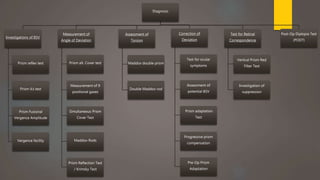
3. Prisms are used in orthoptics to diagnose and manage ocular deviations and binocular vision disorders through tests like the prism reflex test, prism alternate cover test, and measurement of fusional vergence amplitudes.





























































![Corneal blindness in a southern indian population [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/cornealblindnessinasouthernindianpopulationautosaved-140211072740-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)





















