primary cutenous lymphoma..
•Download as PPTX, PDF•
0 likes•225 views

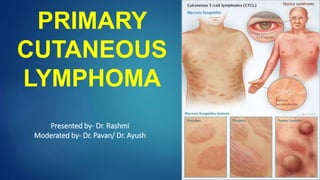
Primary cutaneous lymphoma is a type of non-Hodgkin lymphoma that presents in the skin without evidence of disease elsewhere. Mycosis fungoides is the most common type of cutaneous T-cell lymphoma, typically presenting as patches or plaques on the skin. Sezary syndrome involves generalized erythema and the presence of malignant T-cells known as Sezary cells in the blood. Treatment depends on the stage of disease and may include skin-directed therapies, phototherapy, chemotherapy, targeted therapies, or total skin electron beam radiation therapy. Prognosis is generally good for early stage mycosis fungoides but poorer for advanced or leukemic forms of the disease such as Sezary syndrome

Recommended
More Related Content
What's hot
What's hot (20)
Similar to primary cutenous lymphoma..
Similar to primary cutenous lymphoma.. (20)
More from Dr.Rashmi Yadav
More from Dr.Rashmi Yadav (10)
Recently uploaded
Recently uploaded (20)
primary cutenous lymphoma..
- 1. PRIMARY CUTANEOUS LYMPHOMA Presented by- Dr. Rashmi Moderated by- Dr. Pavan/ Dr. Ayush
- 4. Introduction Accumulation of malignant Lymphoid cells in the skin without evidence of extracutaneous disease at the time of presentation. Important to distinguish it from Nodal Lymphoma with skin infiltration
- 8. In western countries annual incidence 1/100000 . Cutaneous T cell lymphoma (CTCL) constitutes 75-80% of all cases Mycosis fungoides is most common CTCL Cutaneous B cell Lymphoma (CBCL) constitutes 20-25% of all cases.
- 9. Mycosis Fungoides Mycosis Fungoides first described in 1806 by Jean- Louis-Marc Alibert in his Atlas of Dermatoses “ description des maladies de la peau” Most common type of CTCL Most common in Males (M:F::1.6-2:1) Median age of presentation 55 to 60 yrs Precise Etiology remains Elusive.
- 10. Cutaneous disease Pruritis in involved area Evolution of skin lesion Premycotic Phase Red scaled macular or patch like lesion in sun shielded areas Unstable and Regress Biopsy not diagnostic b/o paucity of Lymphocytes Patch Phase Any size lesion without induration or significant elevation above the surrounding uninvolved skin Poikiloderma may be present
- 11. Plaque Phase ( dense infiltration by malignant cells ) Any size lesion that is elevated or indurated Crusting or poikiloderma may be present Tumor Phase Plaque may evolve into cutaneous tumor Any solid or nodular mass > 1 cm in diameter with evidence of deep infiltration in the skin and /or vertical growth MF may also progress or present with erythroderma
- 14. Leukemic CTCL and Sezary Syndrome (SS) – In rare CTCL cases circulating malignant T-cells are identified in peripheral blood. Most commonly occurs in association with erythroderma but may occur in patient with minimal cutaneous disease CD4+/CD7- or CD4+/CD26- immunophenotype – Disease burden is explained by B staging. Distinction between Erythrodermic MF with leukemic involvement and SS is a controversy SS defined as combination of erythroderma with B2 disease.
- 15. involvement of regional lymph nodes (approximately 30 percent in MF ) Lungs Spleen Liver Gastrointestinal tract. Bone marrow involvement is rare Progression to Extracutaneous disease correlates withextent of skin disease Limited patch or plaque very rare Generalized plaque- 8 % Tumorous or generalized erythroderma-30-40% Hence, extracutaneous is more commonly seen in Sezary syndrome.
- 16. Molecular pathology of Mycosis Fungoides CD4+ T-HELPER CELLS CD3+ CD4+ CD45RO+ CLA+ CCR4+
- 17. Diagnosis History and physical examination Duration, Evolution, % Area involved Presence or Absence of cutaneous tumor Evaluation of Lymphatic system Appropriate images of cutaneous lesion as guide for therapy response . Skin Biopsy From minimum two distinct sites Excisional biopsy from LN (priority should be given to largest LN with SUV max.)
- 18. Laboratory and imaging studies CBC LFT LDH Peripheral blood examination (Extracutaneous disease) Immunophenotype (CD 2+,3+,4+,5+,45RO+,8-,30-) PCR for T-cell receptor gene reassortment Bone marrow biopsy (Extracutaneous disease) CT scan Chest, Abdo. ,Pelvis (Except patch/plaque/limited disease) PET-CT > CT Scan.
- 19. EORTC Diagnostic algorithm: Point based system A total of 4 points is required for the diagnosis of MF based on any combination of points from the clinical, histopathologic , molecular , and immunopathologic criteria. Clinical Findings Skin Biopsy ( Histopathology) Molecular criteria Immunophenotyping : CD3+, CD4+, CD8-, CD30-, CD45RO+, TCR gene rearrangements
- 27. Goals of treatment are symptom relief and cosmetic improvement (palliation) Early aggressive therapy results in high complete remission rates but no significant difference in DFS or OS. Patients are susceptible to infections with skin flora; immune suppression is undesirable
- 28. Skin Directed Phototherapy : UVB (Ultraviolet B) or PUVA ( Psoralen + UVA photochemotherapy) Topical chemotherapy :- Nitrogen Mustard (HN2) or Carmustine (BCNU) Radiation therapy ( Electron Beam Therapy, TSEBT – Total Skin Electron Beam Therapy) Topical Retinoids ( Baexarotene) Topical Corticosteroids
- 29. Systemic Photopheresis Biologic Therapies : ( IFN alfa) Retinoids/Rexinoids ( Oral Bexarotene or Isotretinoin) HDAC ( Histone Deacetylase inhibitors) - Vorinostat Chemotherapy ( Single agent chemotherapy – Methotrexate, Gemcitabine, Chlorambucil, Cyclophosphamide)
- 30. Local Superficial Irradiation Used in early Stage 1a MF Single abutting Radiation fields are used Treatment fields should be designed to encompass the entirety of the lesion (determined by visual inspection, palpation, and/or appropriate imaging) 1- to 2-cm margin is given lead or Cerrobend cut out are used to conform field borders EORTC recommends that the 80% isodose line is set at the deep border of the dermis approx 4.5mm S/E :- mild dermatitis, local alopecia, and pigmentation changes. Radical dose 30-36Gy and 8Gy in 2 # for Palliation.
- 31. Ingestion of 8-methoxypsoralen (0.6mg/kg, 2hours before UVAexposure) Becomes activated when exposed to UV light and increases the skin's sensitivity to UV light and hence, improves the effectiveness of UV light therapy
- 32. Treatments 3x/wk with subsequent tapering 65% Complete Response, 95% OR, duration ofresponse 43 months, Mean survival 8.5 years in Stage I Adverse effects : nausea, erythema, pruritis, dry skin, secondary skin malignancies
- 33. Nitrogen Mustard (HN2) orCarmustine (BCNU) Overall Response Rates 70-90% in Stage Idisease Adverse effects: contact dermatitis,erythema, telangiectasias
- 34. Reserved for Sezary Syndrome Technique: Patient ingests 8-MOP. Leukapheresis, mononuclear fraction of patient‘s WBCs are collected and exposed to UVA, then returned to patient. UVAis toxic to cells and reinfused cells stimulate a selective immune response against malignant cells. RR (response rate) 73%, median survival 5years in one study of pt‘s with mainly SS
- 35. ORR 79% in pts with all stage disease Maximum dose limited by side effects Started at 3million U and titrated up t omaximum of 15million U 3x/wk In one study combining PUVA with IFN 1 2million Units 3x/wk – ORR 88%, CR 62%, response duration 28 months
- 36. Novel Retinoid – Rexinoid FDA approved for use in advanced MF i.e; Stage IIB to IVB in patients who have not responded to at least one prior systemic therapy Selectively activates retinoid X receptors Acts on retinoid response elements t oalter gene expression
- 37. Adverse effects: Hypertriglyceridemia 63% Most patients require drugs to reduce hypertriglyceridemia such as statin or fibrates. Diet should include Vitamin E and dietary consultation, especially for monotherapy patients. Hypothyroidism 43% These patients need synthroid supplements. Leukopenia 7% Dose adjustments control leukopenia Teratogenic
- 38. Chemotherapy
- 39. CTCL is very radiosensitive Use of Electron Beam Therapy limits toxicity Standard total dose is 36 Gy CR 56-96% in Stage IA-IIA Given in combination with other agents toavoid relapse Toxicity: erythema, pain, swelling, hairand nail loss, secondary skin cancer
- 40. TSEBT (Total Skin Electron Beam Therapy ) Technique :- Accomplished with 6- to 9-MeV electrons Patient standing behind a polycarbonate screen ~3.8 meters from the linear accelerator head Treatment is provided in “cycles,” with one cycle composed of treatment of the patient in six different positions over 2 days (three positions each day) A dual-field technique is used to deliver treatment to a superior and inferior field by angling the gantry 16 to 17.5 degrees above and below horizontal. Six position treatment deliver maximum dose to a depth of 1mm, 80% dose to 6-7mm. A 3.2-mm polycarbonate screen (Lexan) is placed in front of the patient which serves to attenuate and scatter the incident electrons, resulting in an electron energy of 3.9 MeV at the skin surface
- 49. Hoppe RT, Kim YH,Clinical features, staging, and prognosis of mycosis fungoides and Sezary syndrome, Uptodate.com, 11/06
- 52. Sezary cells are mononuclear cells with acerebriform nucleus Small numbers of these cells can be seen among healthy individuals In MF,an increased number of Sezary cells seen in the peripheral blood. An absolute count ≥1000 Sezary cells/cubic mm is a diagnostic criterion for Sezary syndrome.
- 53. Circulating Sezary Cell This Sezary cell is the malignant pleomorphic T cellseen in mycosis fungoides and has a convoluted nucleus
- 54. Cerebriform nuclei of Sezary cell
- 55. Generalized erythroderma + intense Pruritis Lymphadenopathy Atypical T- cells (Sezary cells) in the peripheral blood (An absolute count ≥1000 Sezary cells/cubic mm is a diagnostic criterion for Sezary syndrome equivalent to the B2 designation in the TNMB classification syndrome). Low levels of Sezary-like cells can bedetected in the peripheral blood of patients with benign skin conditions. Hence, diagnostic criteria of Sezary syndrome uses an absolute Sezary cell count of >1000/microL with positive clones
- 56. Diagnosis is made when there is a clonal rearrangement of the T-cell receptor (TCR) in the blood (identified by PCR or southern blot analysis) plus either an absolute Sezary cell count of at least 1000 cells/microL or one of the following two criteria Increased CD4+ or CD3+ cells with a CD4 to CD8 ratio of 10 or more. Increased CD4+ cells with an abnormal phenotype (such as a CD4+ to CD7- ratio ≥40 percent or a CD4+ to CD26- ratio ≥30 percent
- 57. Treatment includes Extracorporeal Photopheresis ( ECP) alone or in combination with other therapies ( IFNα) OR 30-80% and CR 15-25%. Recent studies report benefitis with Bexarotene and Alemtuzumab (anti-CD52) therapies – more data needed. Prognosis - generally poor with a median survivalbetween 2 and 4 years. Most patients die of opportunistic infections thatare due to immunosuppression
- 58. Thank You
Editor's Notes
- 1st case of MF 1806 After Alibert released his depiction of MF, approximately 300 similar cases were reported over the next decade, and in modern times, approximately 1,500 new cases of MF were diagnosed during 2001 to 2005
- CADM1 diagnostic marker