The document discusses the prevalence and impact of medical errors, particularly in the laboratory testing process, highlighting that 60-70% of medical decisions are based on lab results. It emphasizes the complexity of the total testing process and identifies common pre-analytical errors that can lead to significant patient injury and increased healthcare costs. The document concludes with recommendations for improving specimen quality and reducing pre-analytical errors through training and adherence to best practices.
Presenting Dr. Normila Abd Hadi from Hospital Kuala Krai, emphasizing the context of medical errors.
Overview of topics including medical errors, laboratory processes, sample issues, and minimizing errors.
Highlighting that medical errors are a major cause of death, with significant statistics reflecting their impact.
Laboratory services are vital in healthcare, impacting diagnosis and treatment decisions significantly.
Describing the comprehensive laboratory testing process from clinical question to decision making.
Defining laboratory errors as defects between test order and result reporting.
Reviewing laboratory errors by phase: pre-analytical, analytical, and post-analytical with respective statistics.
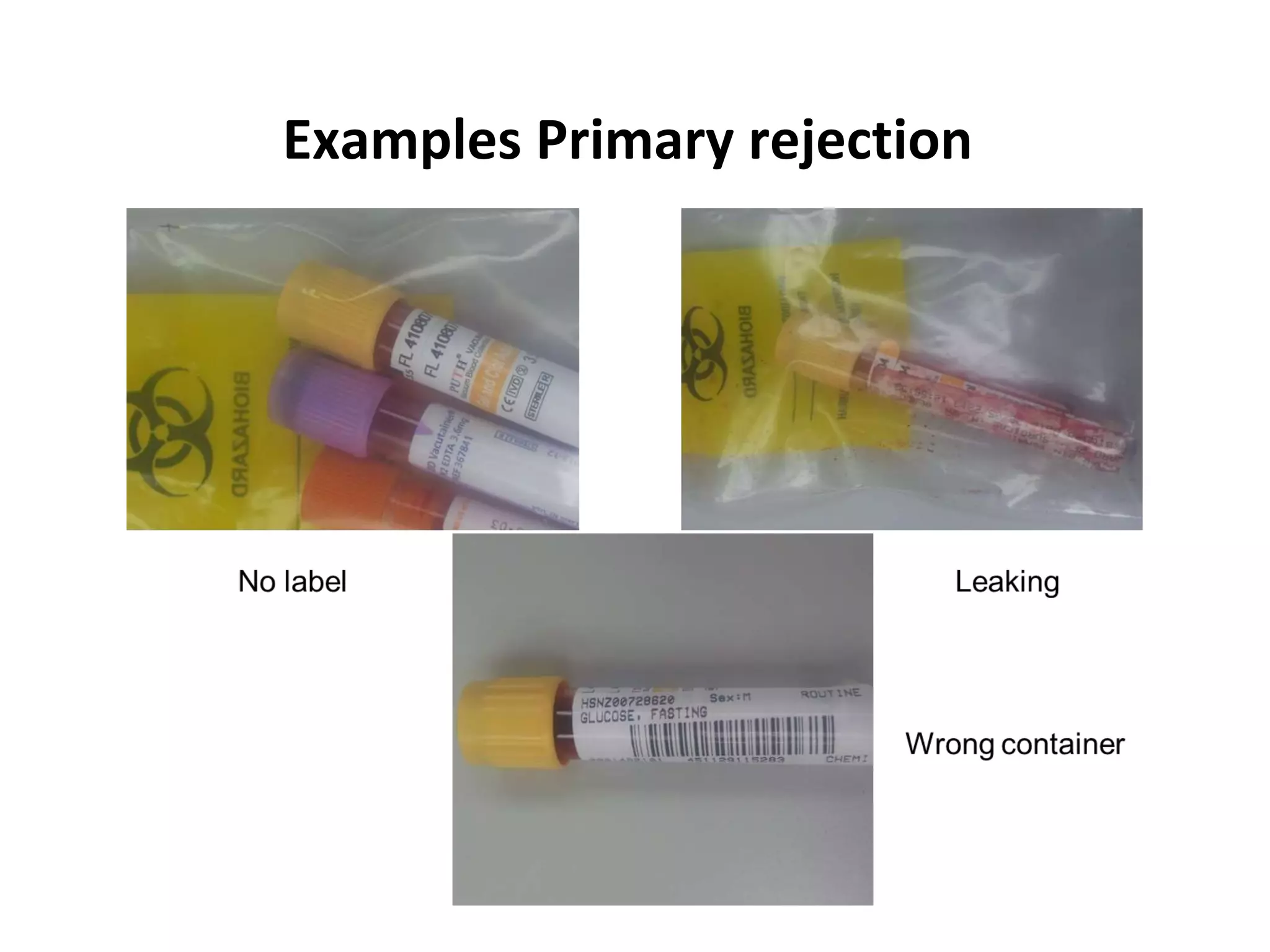
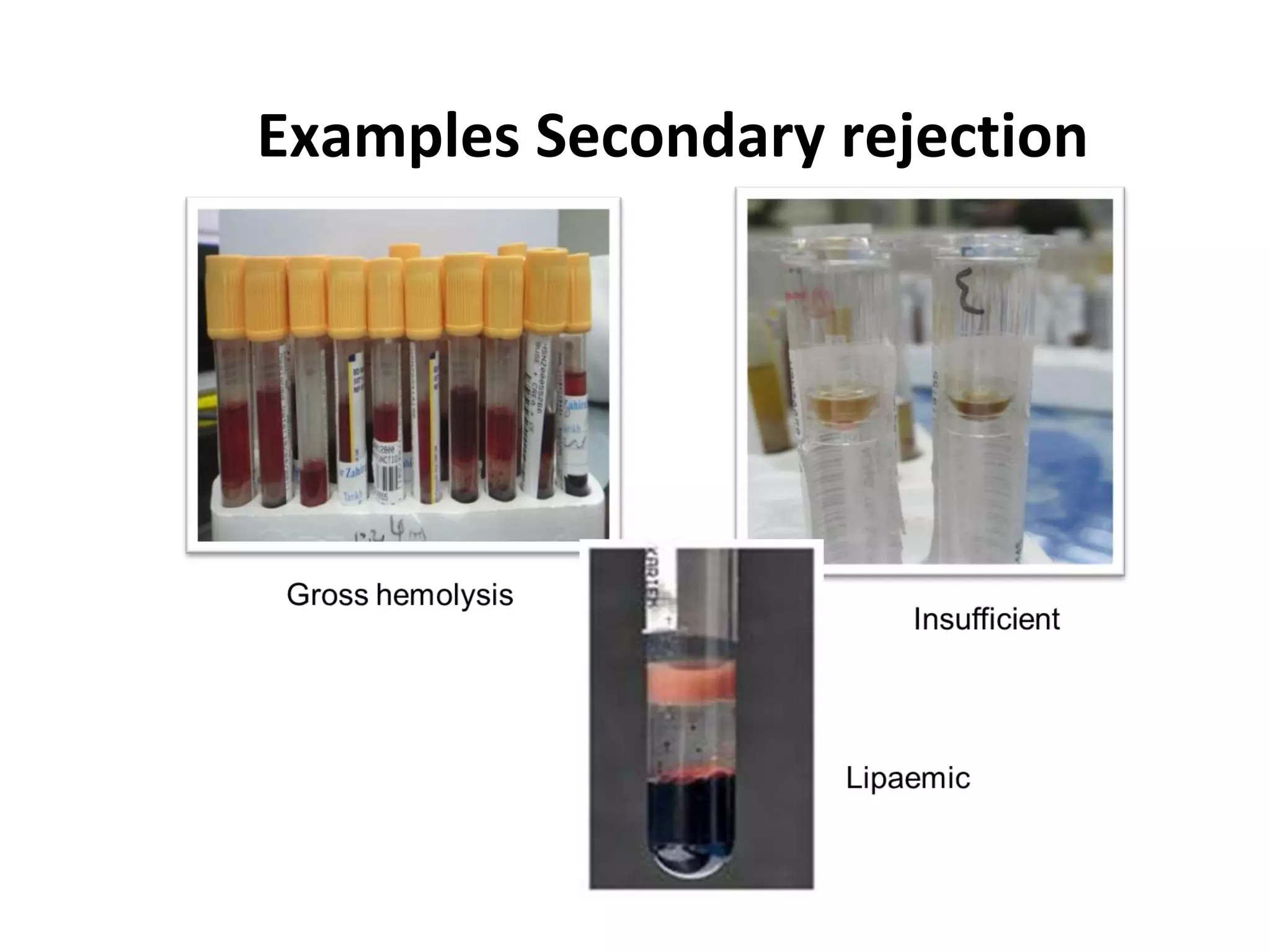
Outline of primary and secondary rejections that occur in laboratory specimens.
Consequences of sample rejection on patient care including delayed diagnosis and increased healthcare costs.
Effects of sample rejection on laboratory operations including turnaround time and additional costs.
Identifying the pre-analytical phase as the most error-prone segment of laboratory processes.
Explaining physiological factors and technical errors contributing to variations in lab analysis.
Common roots of pre-analytical errors such as hemolysis, identification errors causing serious consequences.
Recommendations for best practices in sample collection to avoid errors in patient identification.
Importance of timed sample collections due to diurnal variations affecting test results.
Defining best and inappropriate sites for venipuncture to prevent sample collection errors.Detailed phlebotomy techniques to prevent sample errors including tourniquet use and order of draw.
Discussing the negative impact of delays in processing samples on test results.
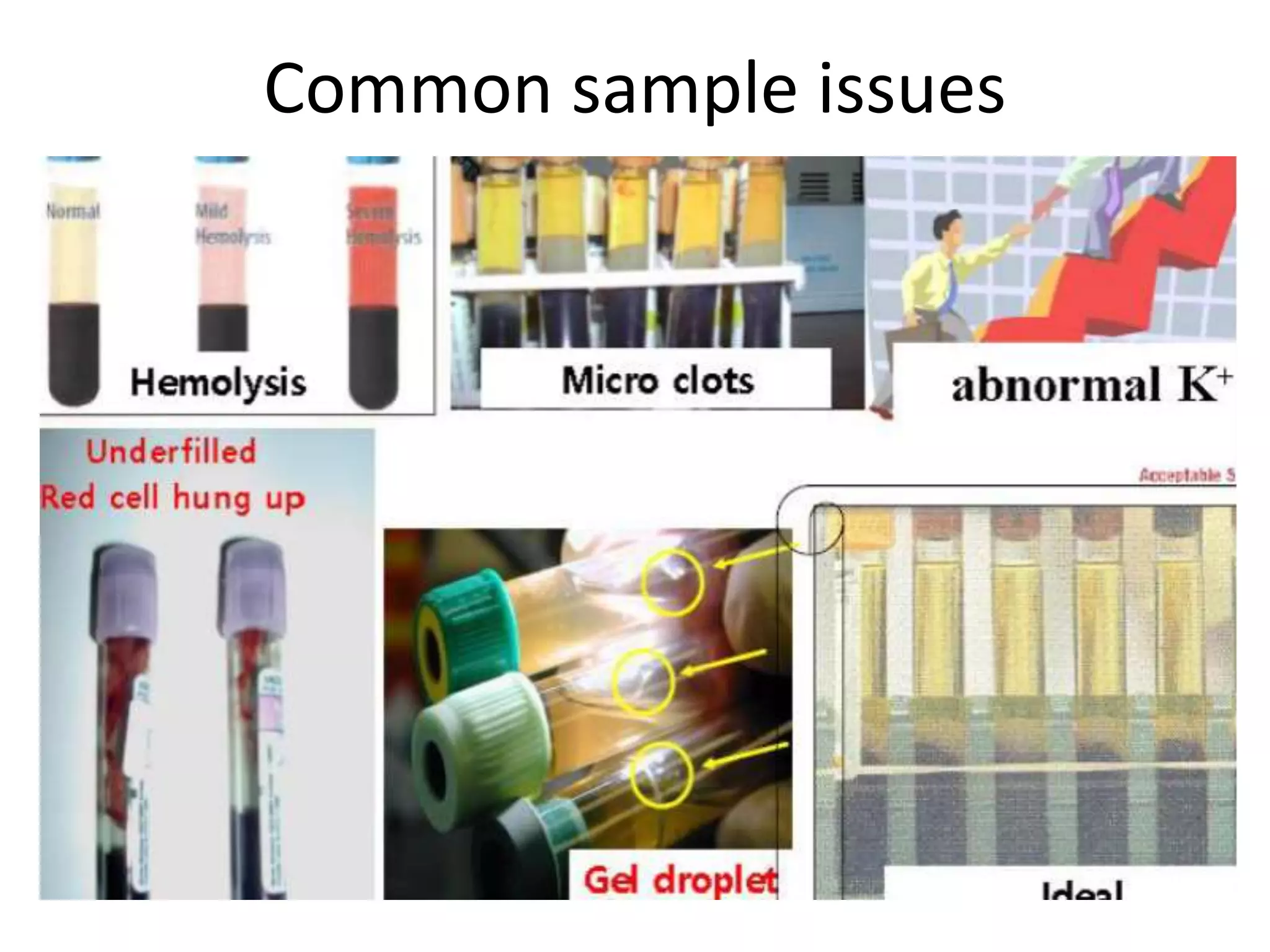
Identifying common sample issues that lead to errors in laboratory results.
Explaining hemolysis, its causes, and testing impacts on results related to RBC breakdown.
Strategies for quality control and staff training to minimize pre-analytical errors.
Importance of standardized training programs to reduce pre-analytical errors in labs.
The reliance on accurate laboratory results for patient management and the importance of quality specimens.
Summary of best practices for specimen handling to avoid laboratory errors.
List of references for studies and literature regarding medical and laboratory errors.
Dr Normila AbdHadi
Department of Pathology & Transfusion
Hospital Kuala Krai
2.
Table content
• Medicalerrors and errors within laboratory
total testing process
• Impact of sample rejection
• Pre analytical variables in laboratory total
testing process
• Common sample issues
• Ways to minimize pre-analytical errors
• Conclusion
3.
Medical Errors
• Thecomplexity of the current healthcare environment has increased
the potential of medical errors.
• Statistics by the Institute of Medicine (IOM):-
– Hospital-based errors is 8th leading cause of death in US
– Medical errors contribute to >1 million injuries and approximately
44k - 98k deaths in hospital annually
– These errors results in 2.4 milion extra days of hospitalization thus
increase hospital costs.
• A study of medical errors published in the New England Journal of
Medicine:
– 11% of patients recieved potential harmful care
– 46% of patients did not recieved the recommended care
4.
Laboratory service &testing
• Laboratory services are the backbone of the modern
healthcare sector.
• Laboratory testing provides essential information used by
physicians.
• An estimated 60-70% of medical decisions are based on
laboratory test results. (Regan M & Forsman R, 2006)
• Lab tests are increasingly important position in
– the diagnostic process
– in monitoring the effect of therapy
– in monitoring health of the individual
5.
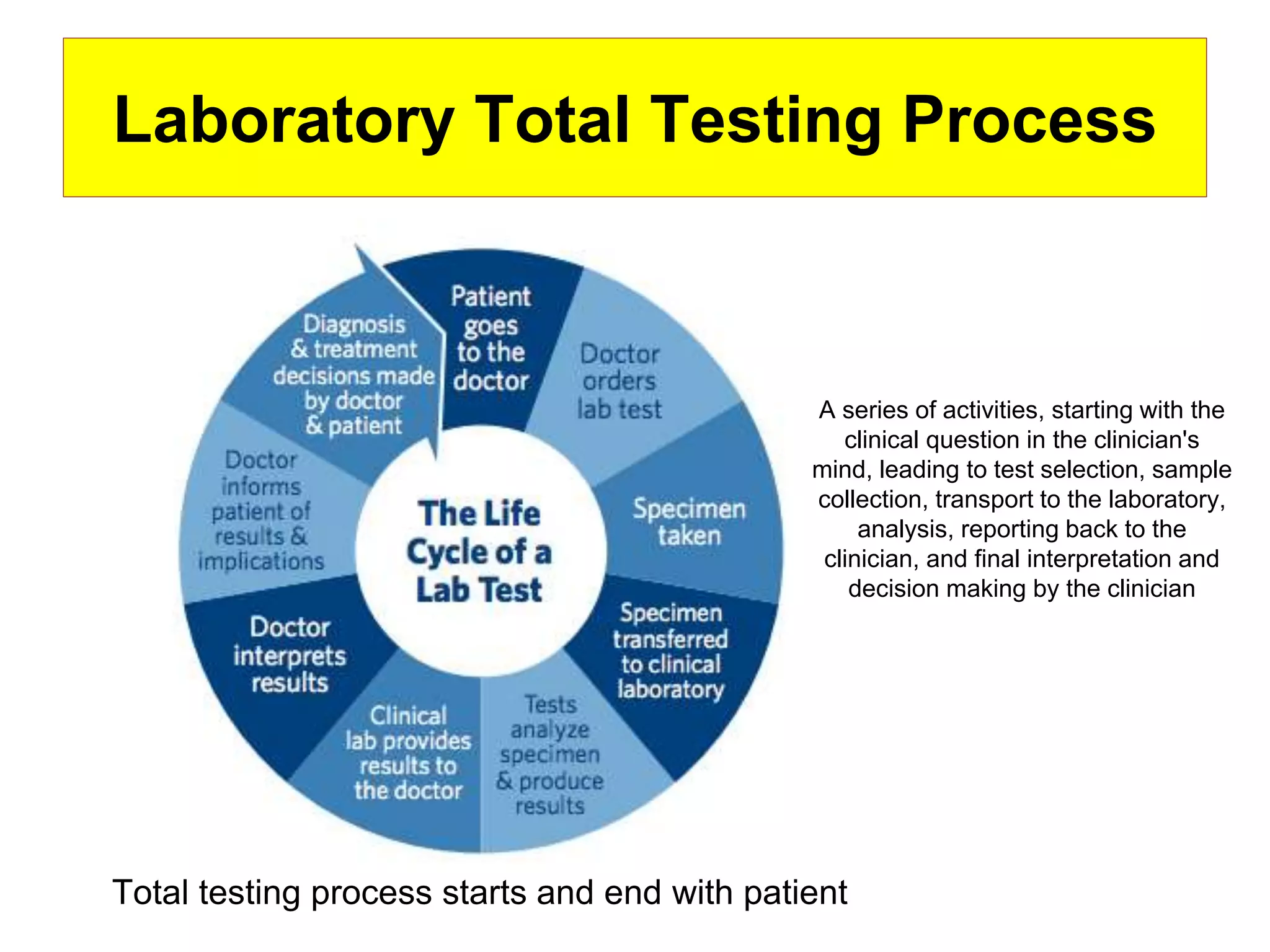
Laboratory Total TestingProcess
Total testing process starts and end with patient
Laboratory Total Testing Process
A series of activities, starting with the
clinical question in the clinician's
mind, leading to test selection, sample
collection, transport to the laboratory,
analysis, reporting back to the
clinician, and final interpretation and
decision making by the clinician
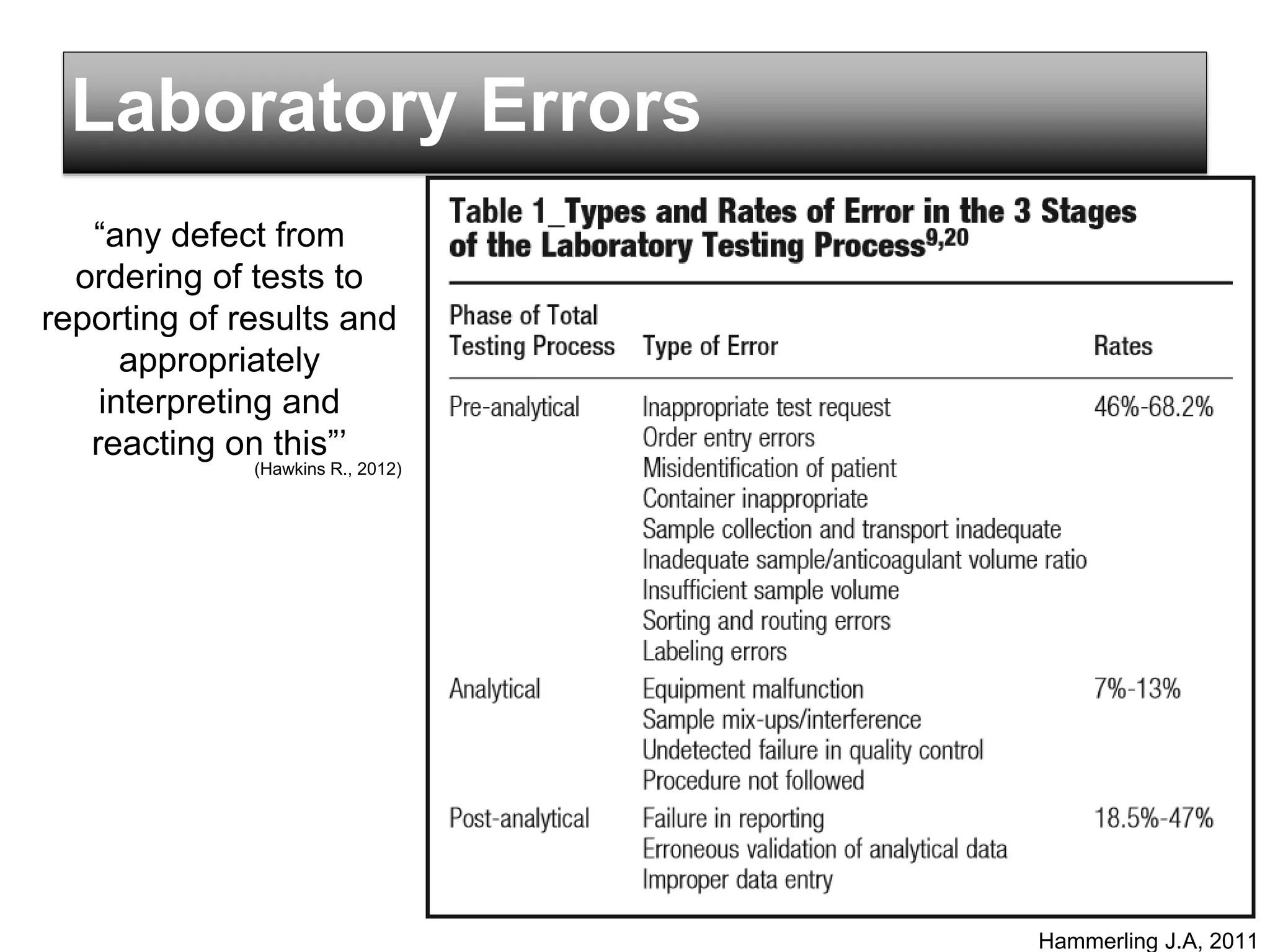
Laboratory Errors
Hammerling J.A,2011
“any defect from
ordering of tests to
reporting of results and
appropriately
interpreting and
reacting on this”’
(Hawkins R., 2012)
8.
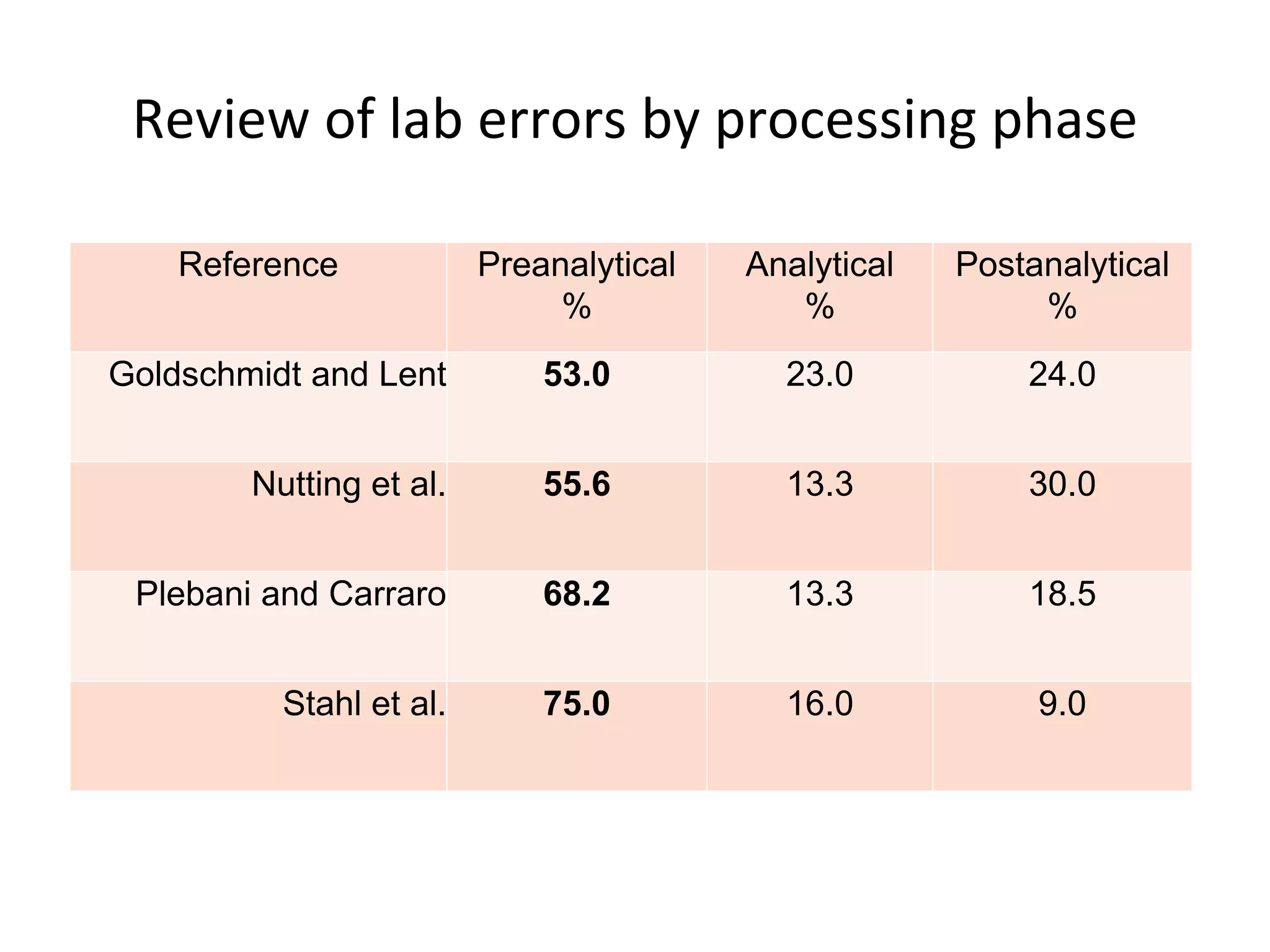
Review of laberrors by processing phase
Reference Preanalytical
%
Analytical
%
Postanalytical
%
Goldschmidt and Lent 53.0 23.0 24.0
Nutting et al. 55.6 13.3 30.0
Plebani and Carraro 68.2 13.3 18.5
Stahl et al. 75.0 16.0 9.0
Impacts of rejection
•Patients
– Delayed diagnosis and treatment
– Misdiagnosed and inappropriate treatment
– Increased risks to patients safety
– Discomfort and stress imposed on patient
– Prolonged hospital stay and increase cost of health care
Sol F. Green “The cost of poor blood specimen quality and errors in preanalytical processes” Clinical Biochemistry 2013
Liyun Cao Et Al. “Causes and Impact of specimen rejection in a clinical chemistry laboratory” Clinica Chimica Acta 2016
12.
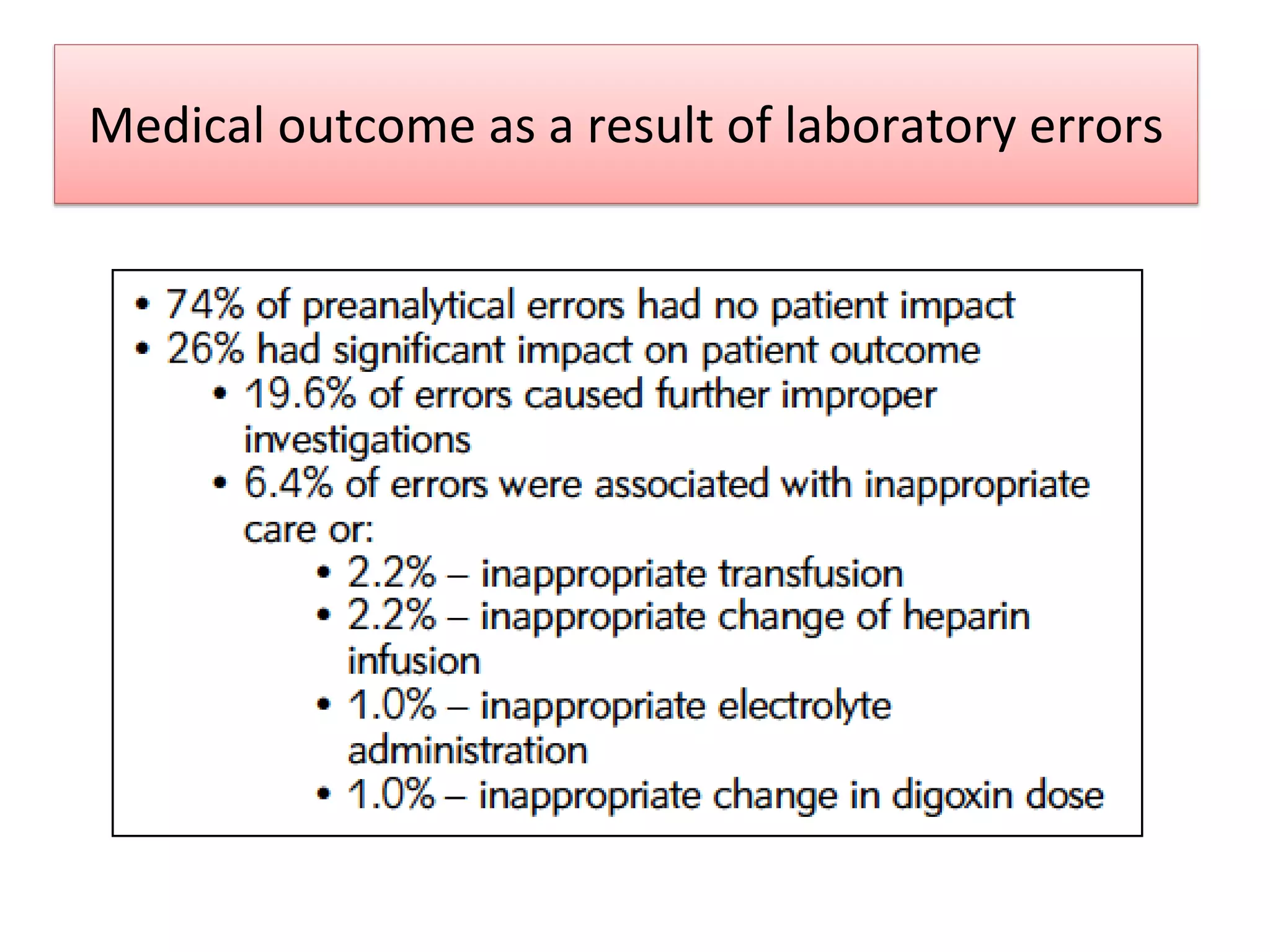
Medical outcome asa result of laboratory errors
Sol Green “Improving the preanalytical process: The focus on specimen quality” Data management and Biostatictics
Journal 2008
13.
Impacts of rejection
•Laboratory
– Prolonged turn around time
– Extra work – communicate between clinicians and lab
personal
– Extra expenditure/cost for recollection and retesting and
reanalysis.
• re-venipuncture
• Cost – syringe, tube, form
• Reagent use
Sol F. Green “The cost of poor blood specimen quality and errors in preanalytical processes” Clinical Biochemistry 2013
Liyun Cao Et Al. “Causes and Impact of specimen rejection in a clinical chemistry laboratory” Clinica Chimica Acta 2016
14.
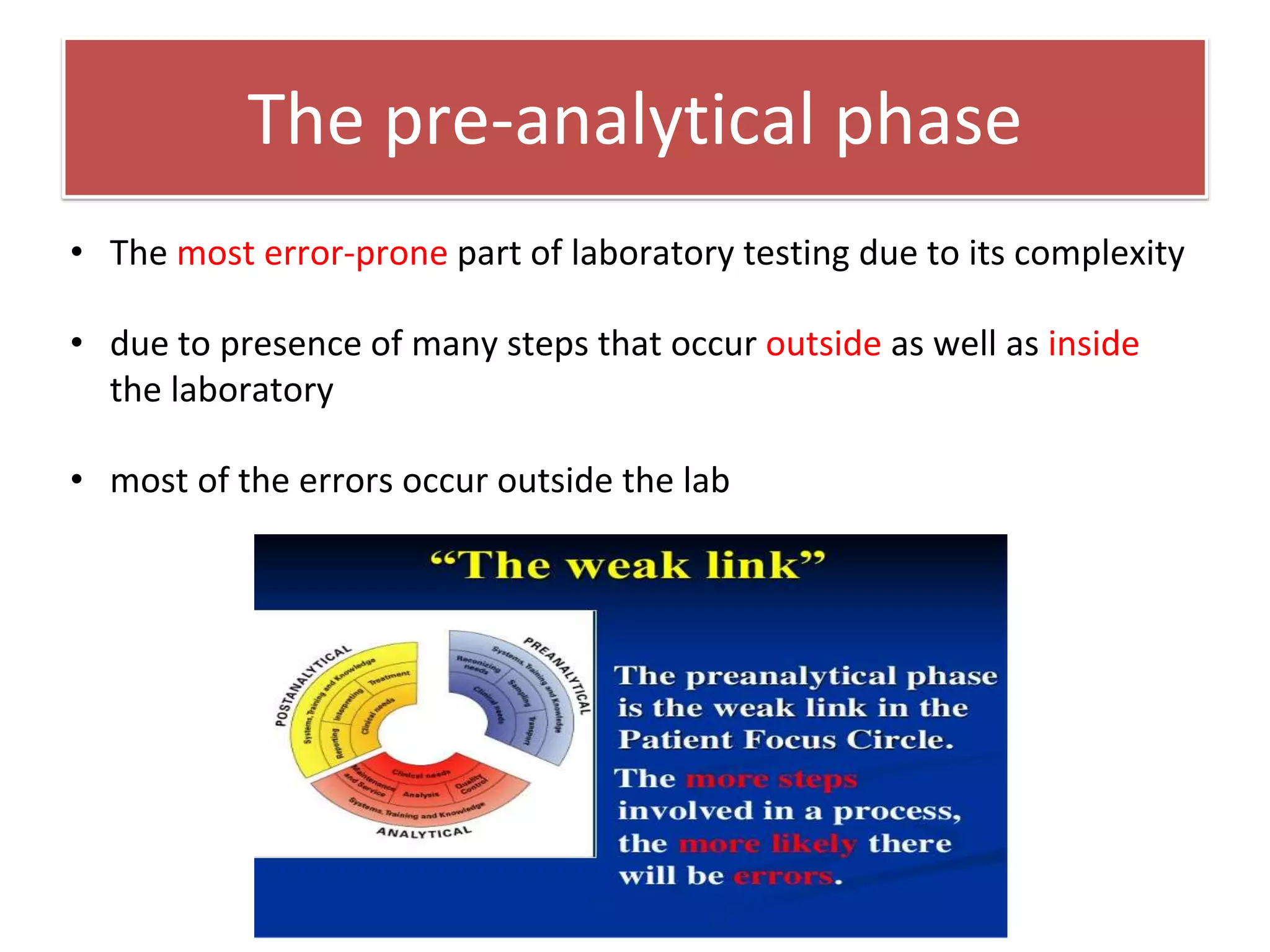
The pre-analytical phase
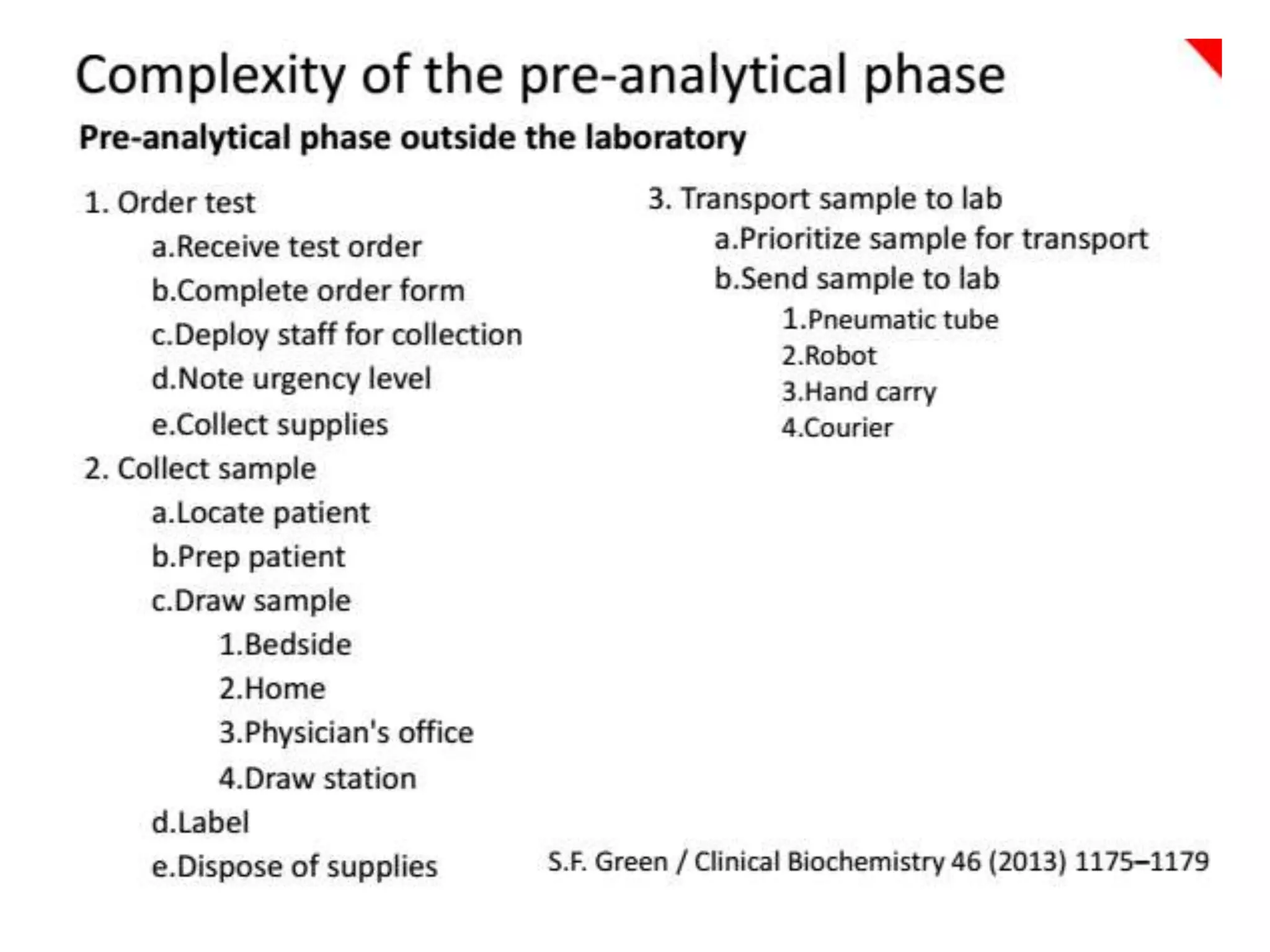
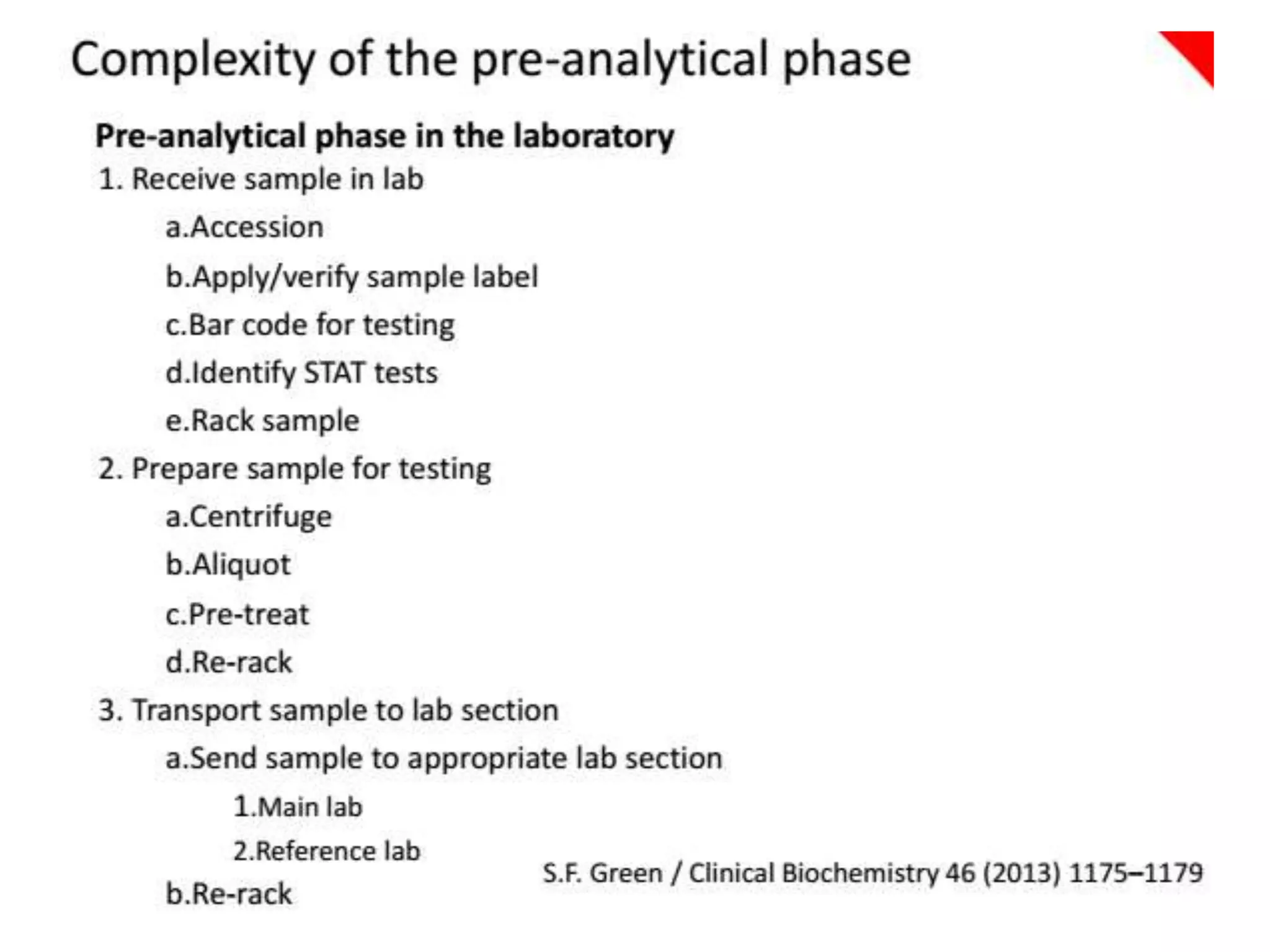
•The most error-prone part of laboratory testing due to its complexity
• due to presence of many steps that occur outside as well as inside
the laboratory
• most of the errors occur outside the lab
17.
Source of PREANALYTICAL variation in
laboratory analysis
• Physiological/biological factor
– Beyond control of phlebotomist/lab staff
• Technical/pre-analytical factor
– Within control of phlebotomist/lab worker
18.
Physiological and biologicalfactors
Beyond
control
Age
Race
Gender
Pregnancy
Diet
Exercise
Environme
nt/ lifesyle
19.
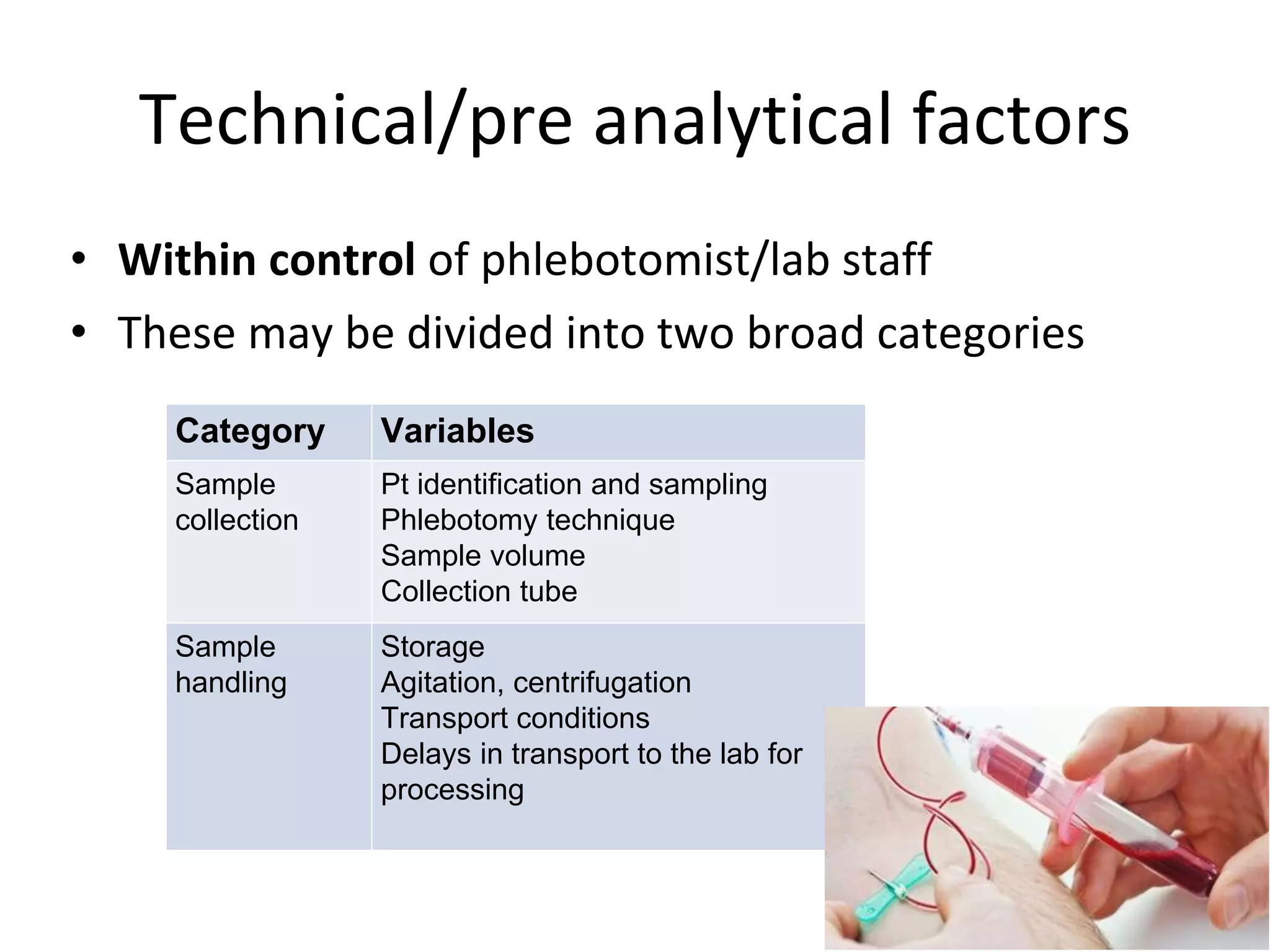
Technical/pre analytical factors
•Within control of phlebotomist/lab staff
• These may be divided into two broad categories
Category Variables
Sample
collection
Pt identification and sampling
Phlebotomy technique
Sample volume
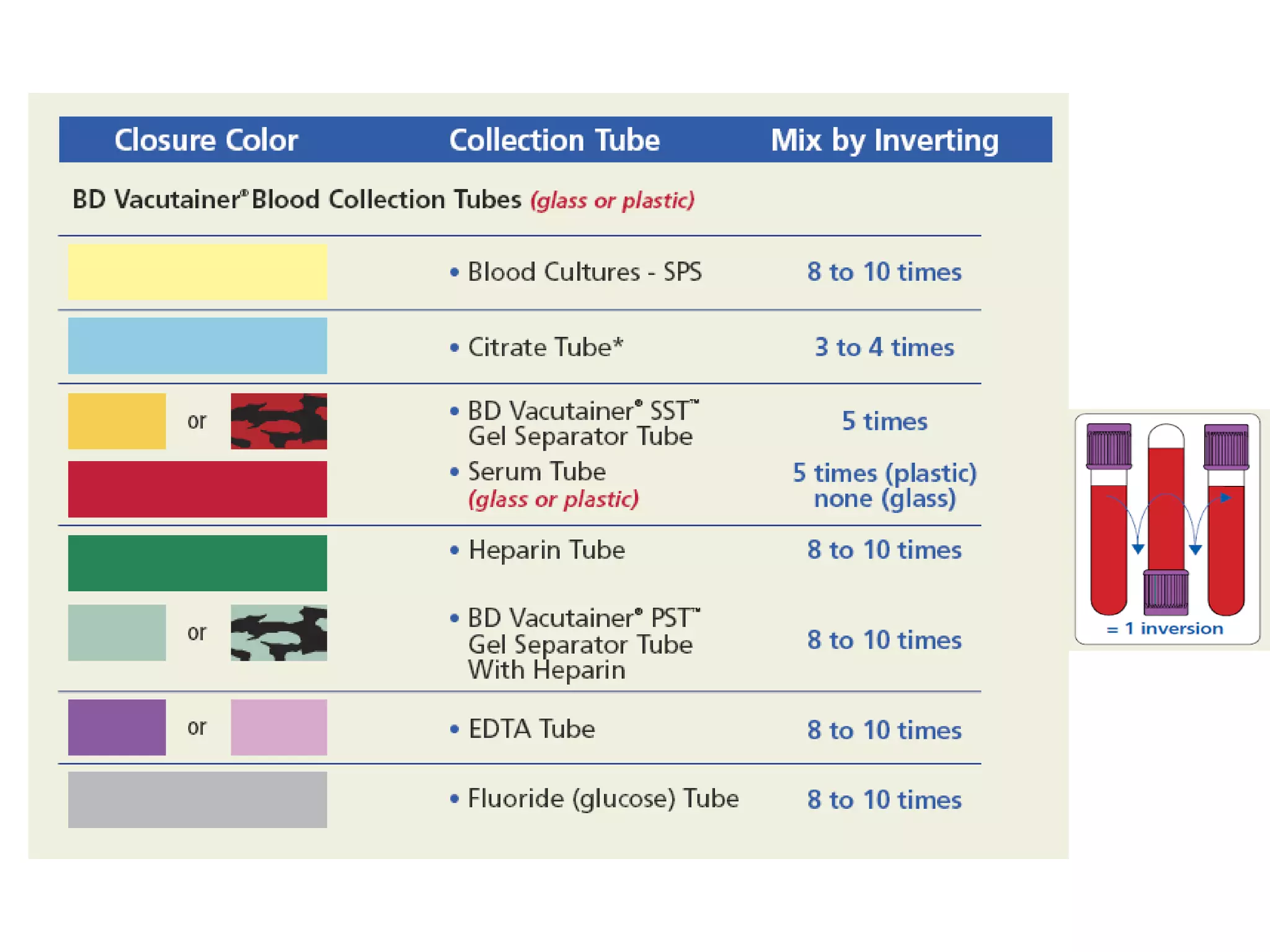
Collection tube
Sample
handling
Storage
Agitation, centrifugation
Transport conditions
Delays in transport to the lab for
processing
20.
Root causes ofPre-analytical variables
• The most frequently encountered causes of
pre-analytical errors are:
• hemolysis
• incorrect patient identification
• insufficient sample volume, and
• clotted specimens
(Salvago et. al J Eval Clin Pract 2008)
21.
Sample collection -Incorrect patient
identification
• Most important steps in venipuncture procedure.
• Incorrect patient identification prior to sample collection
– is one of the major & most dangerous source of pre-analytical
error.
• This can result in
• may be fatal if an acute haemolytic transfusion reaction
occured.
• delayed diagnosis
• additional lab testing
• treatment of a patient for the wrong medical condition
22.
...Incorrect patient identification
Outpatients: to be asked of full name. This is verified
with the information on the request form
Inpatients : check identification band to verify name
and hospital identification number match
to the order
Young or mentally
incompetent
patient
: need to ask patient’s parent, relative or
nurses in-charge to identify him/her
23.
• Best practice:
–Draw and label the specimen at the bedside
– Do not label tube prior to venipuncture
– The outpatient must not be dismissed before labelling is
complete
– Make sure the information on the request form and sample
are tally
...Incorrect patient identification
24.
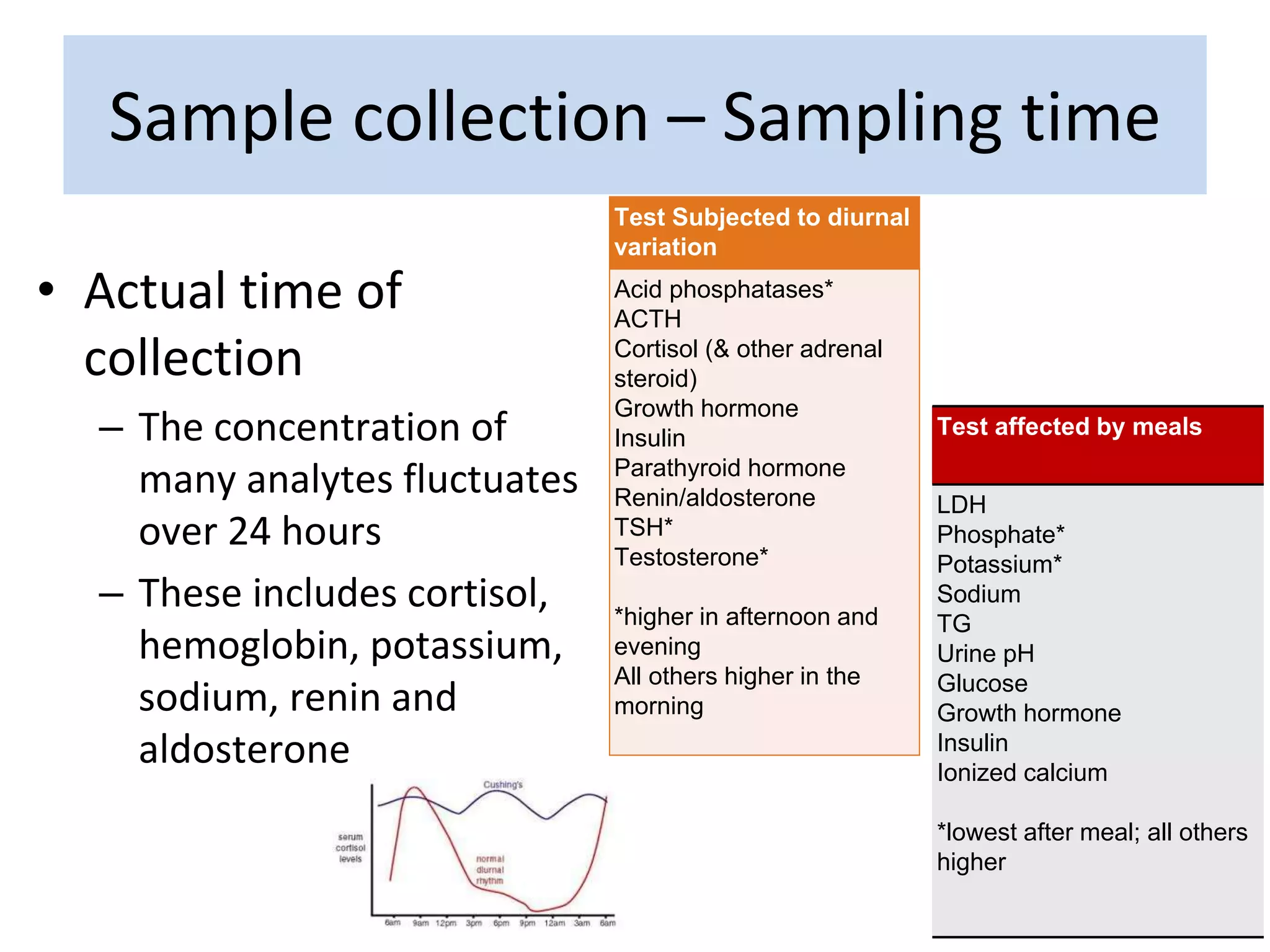
• Actual timeof
collection
– The concentration of
many analytes fluctuates
over 24 hours
– These includes cortisol,
hemoglobin, potassium,
sodium, renin and
aldosterone
Test Subjected to diurnal
variation
Acid phosphatases*
ACTH
Cortisol (& other adrenal
steroid)
Growth hormone
Insulin
Parathyroid hormone
Renin/aldosterone
TSH*
Testosterone*
*higher in afternoon and
evening
All others higher in the
morning
Test affected by meals
LDH
Phosphate*
Potassium*
Sodium
TG
Urine pH
Glucose
Growth hormone
Insulin
Ionized calcium
*lowest after meal; all others
higher
Sample collection – Sampling time
25.
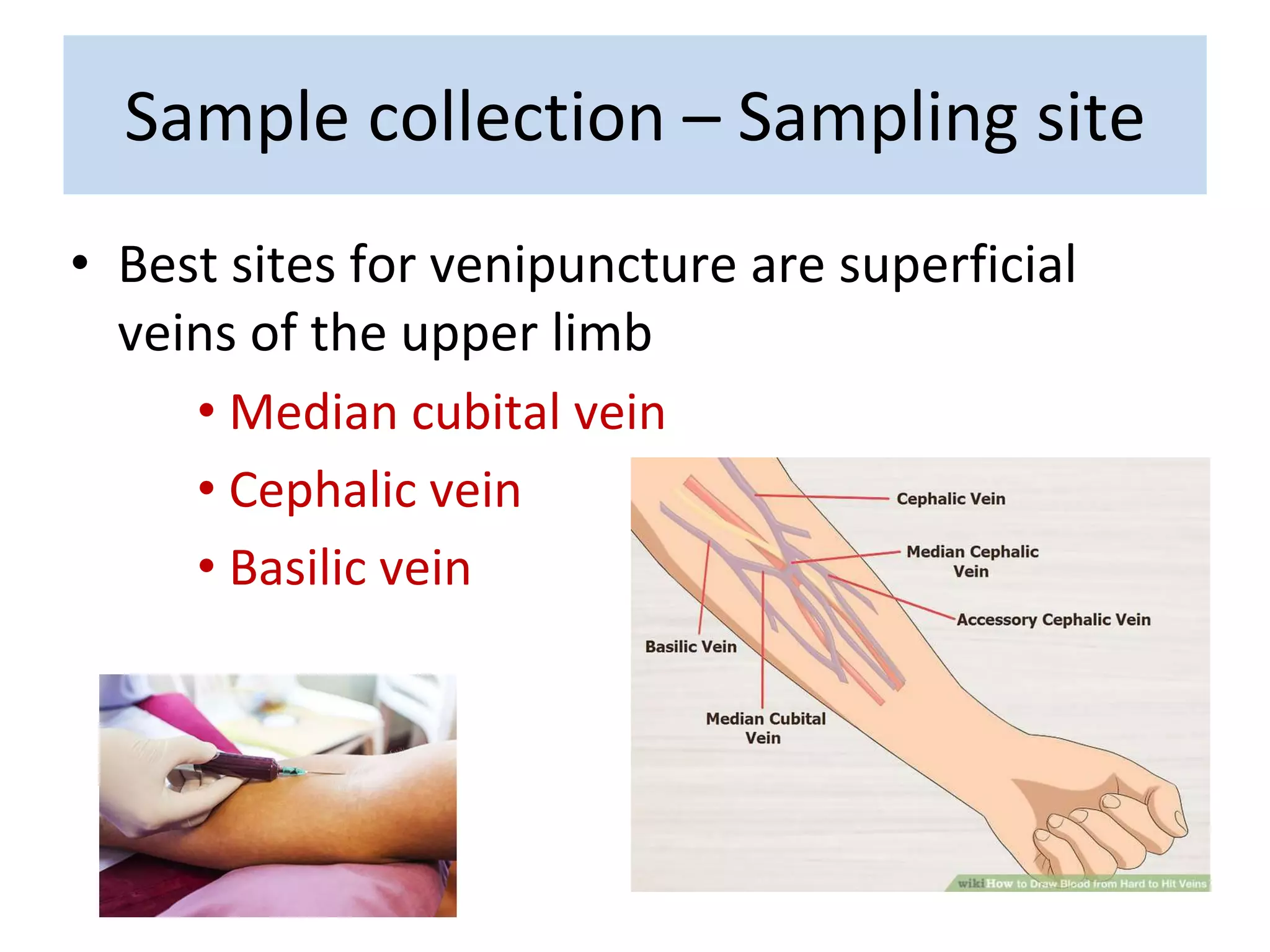
• Best sitesfor venipuncture are superficial
veins of the upper limb
• Median cubital vein
• Cephalic vein
• Basilic vein
Sample collection – Sampling site
26.
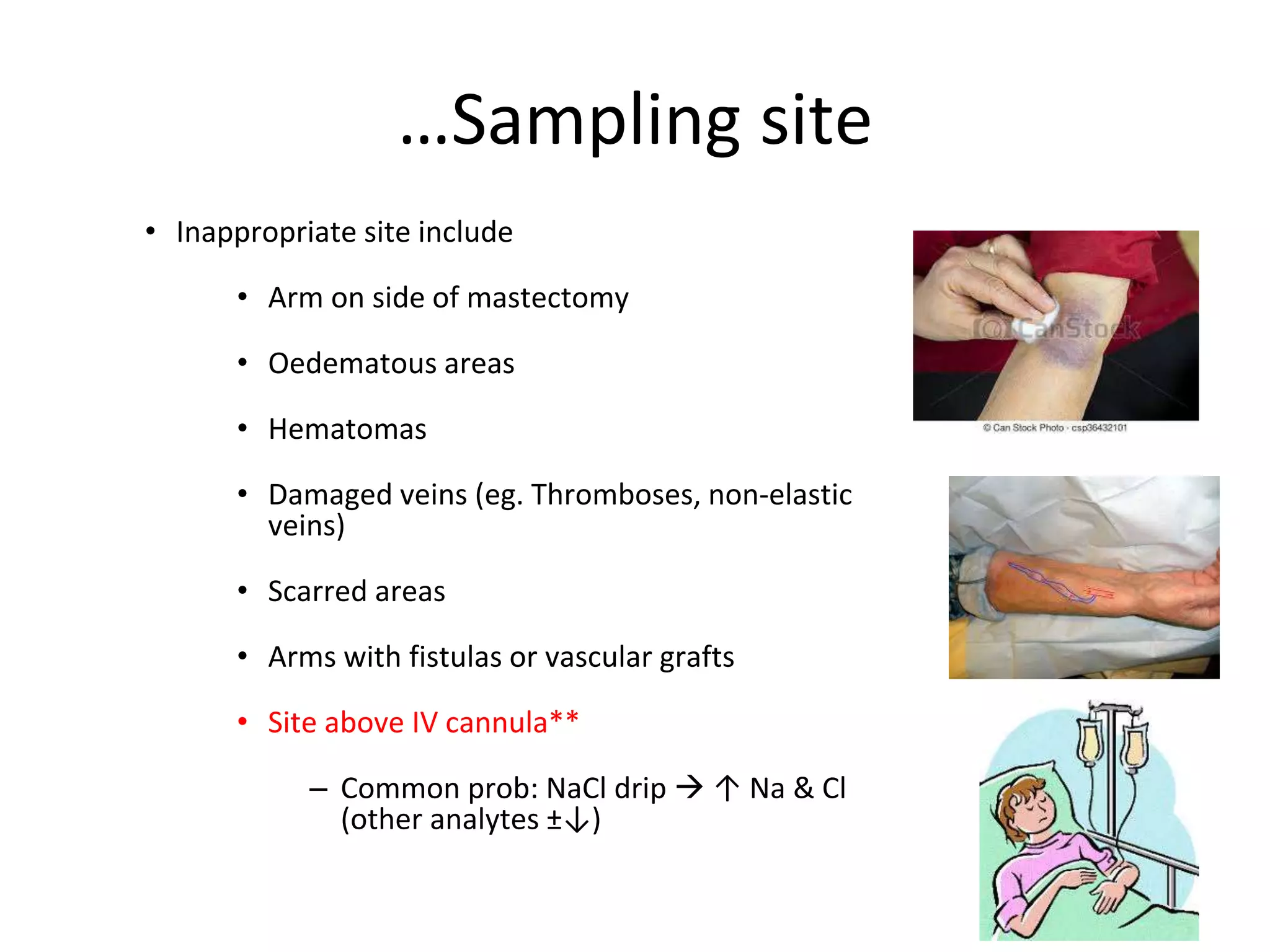
• Inappropriate siteinclude
• Arm on side of mastectomy
• Oedematous areas
• Hematomas
• Damaged veins (eg. Thromboses, non-elastic
veins)
• Scarred areas
• Arms with fistulas or vascular grafts
• Site above IV cannula**
– Common prob: NaCl drip ↑ Na & Cl
(other analytes ±↓)
…Sampling site
27.
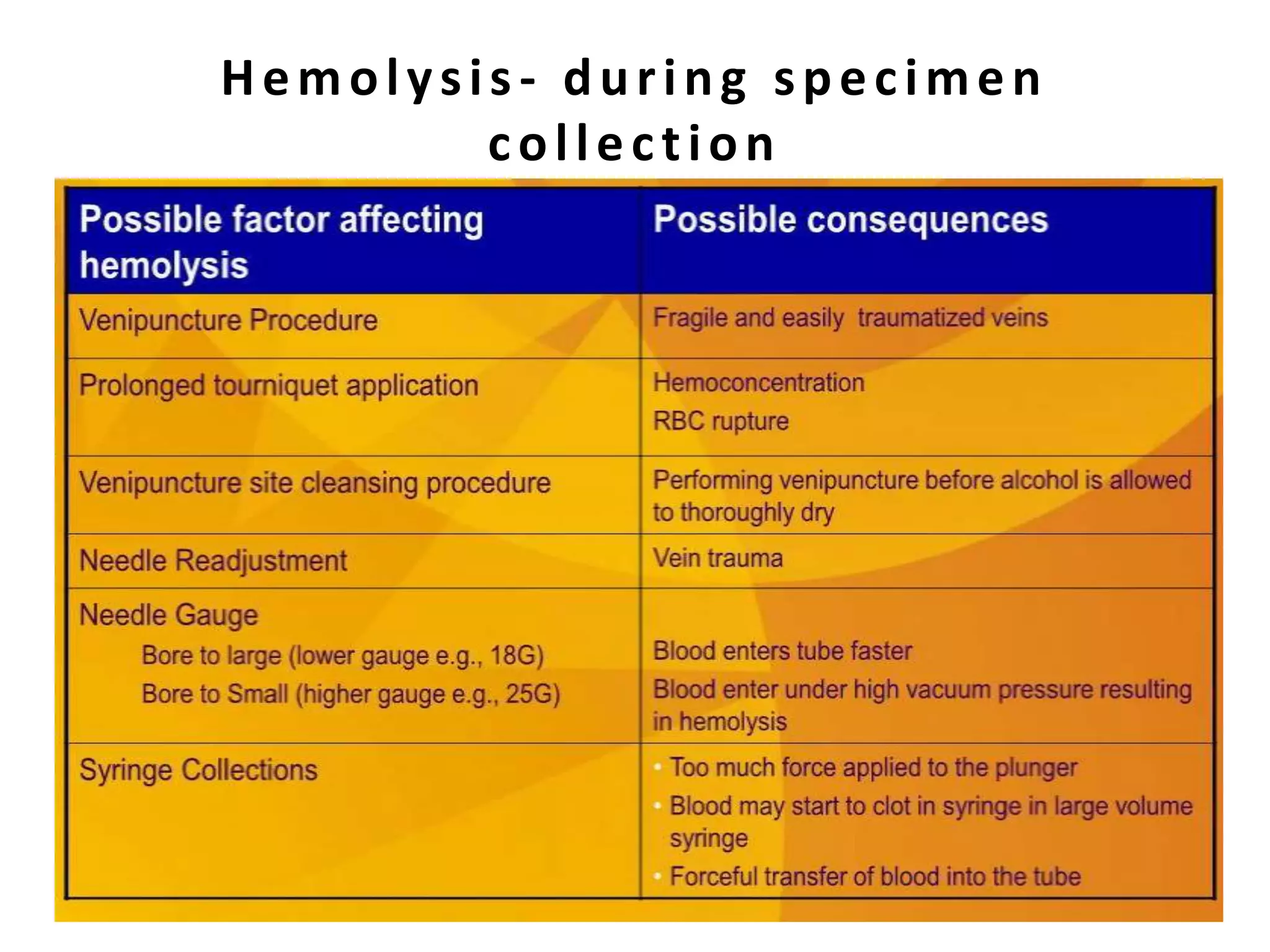
1. Tourniquet applications
–Aim for max application time of 1 minute
• to avoid localised stasis with haemoconcentration
increased Alb, T.protein & protein-bound analytes ( e.g
Calcium, Tbili, Chol, iron)
2. Inappropriately narrow gauge needle leading to clotting & haemolysis
of sample
3. Allow alcohol to dry before sample collection leading to haemolysis
Sample collection – Phlebotomy
technique
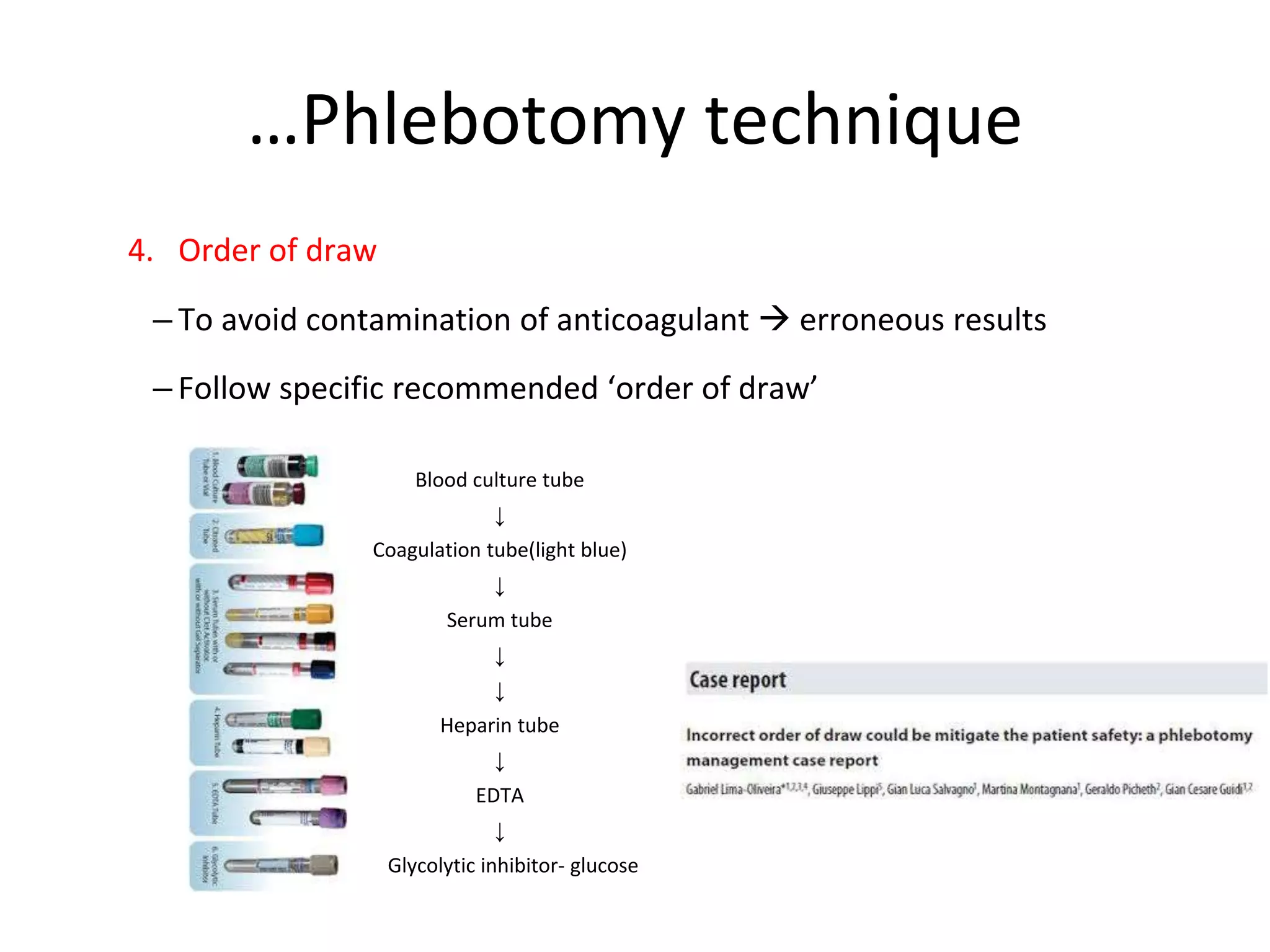
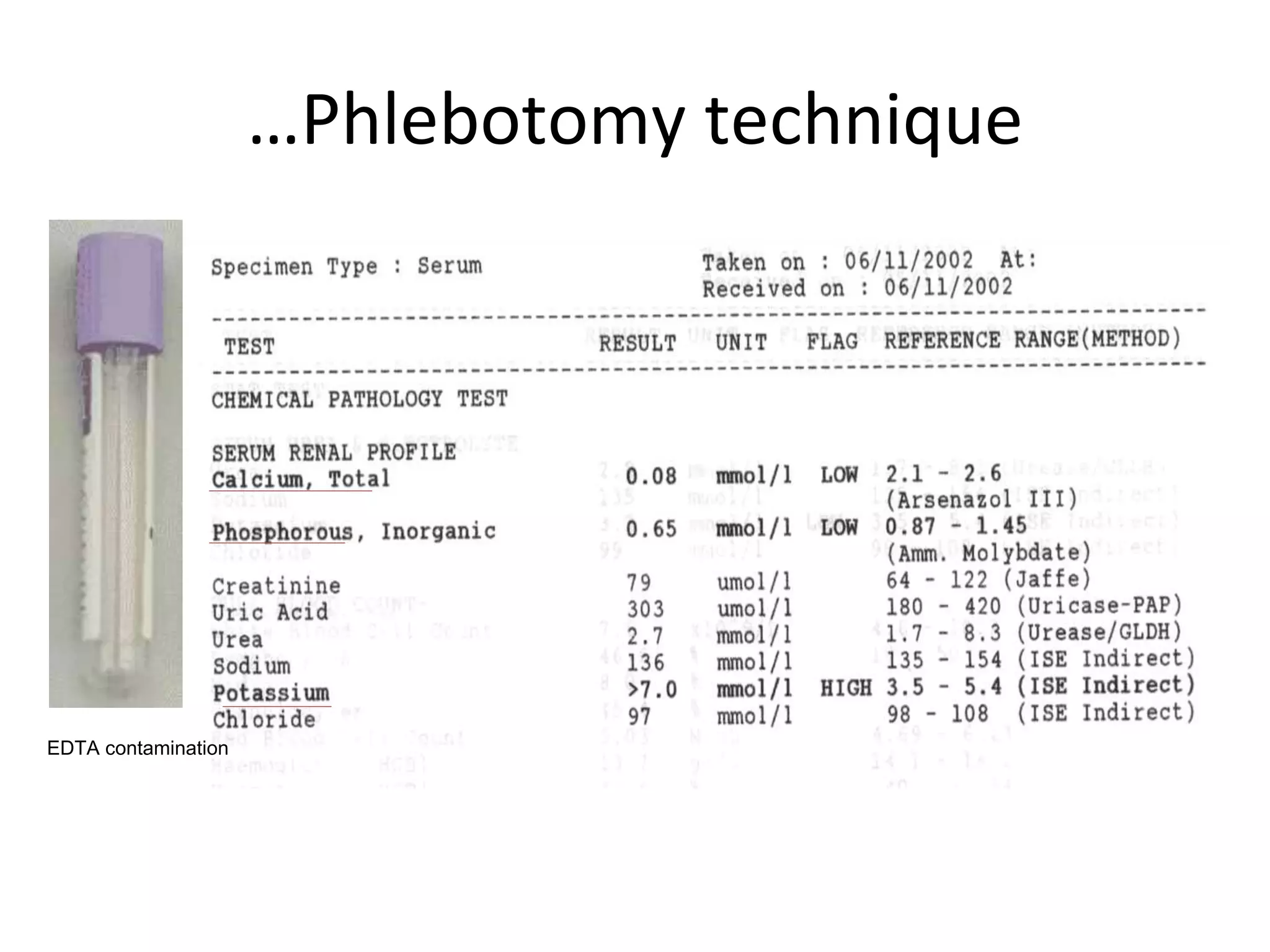
…Phlebotomy technique
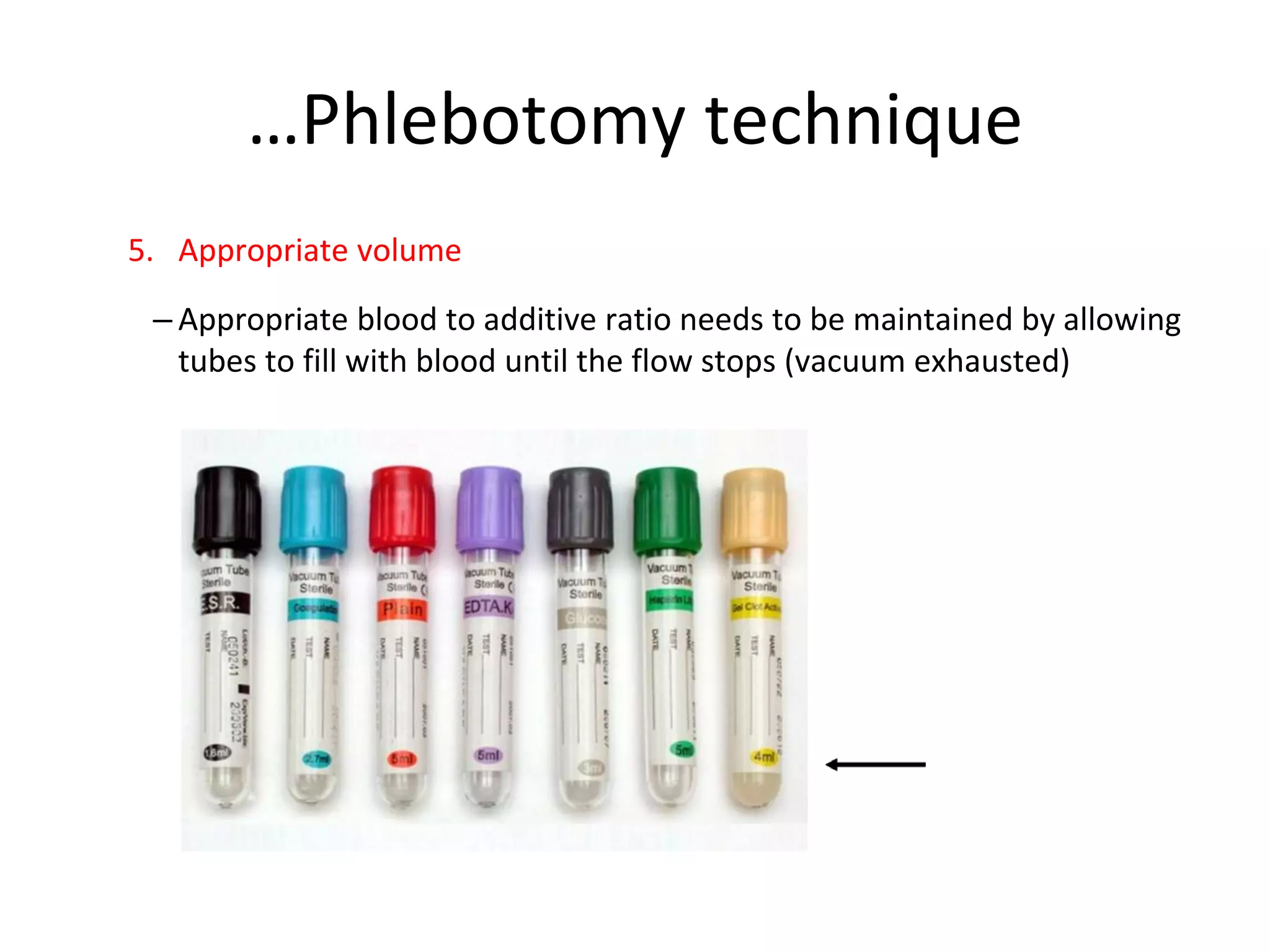
5. Appropriatevolume
– Appropriate blood to additive ratio needs to be maintained by allowing
tubes to fill with blood until the flow stops (vacuum exhausted)
31.
Correct volume ofblood drawn
• Crucial in ensure sufficient sample for analysis
• Also to avoid under filling or over filling volume
impact
• Insufficient sample is one of commonest cause for
rejected sample
32.
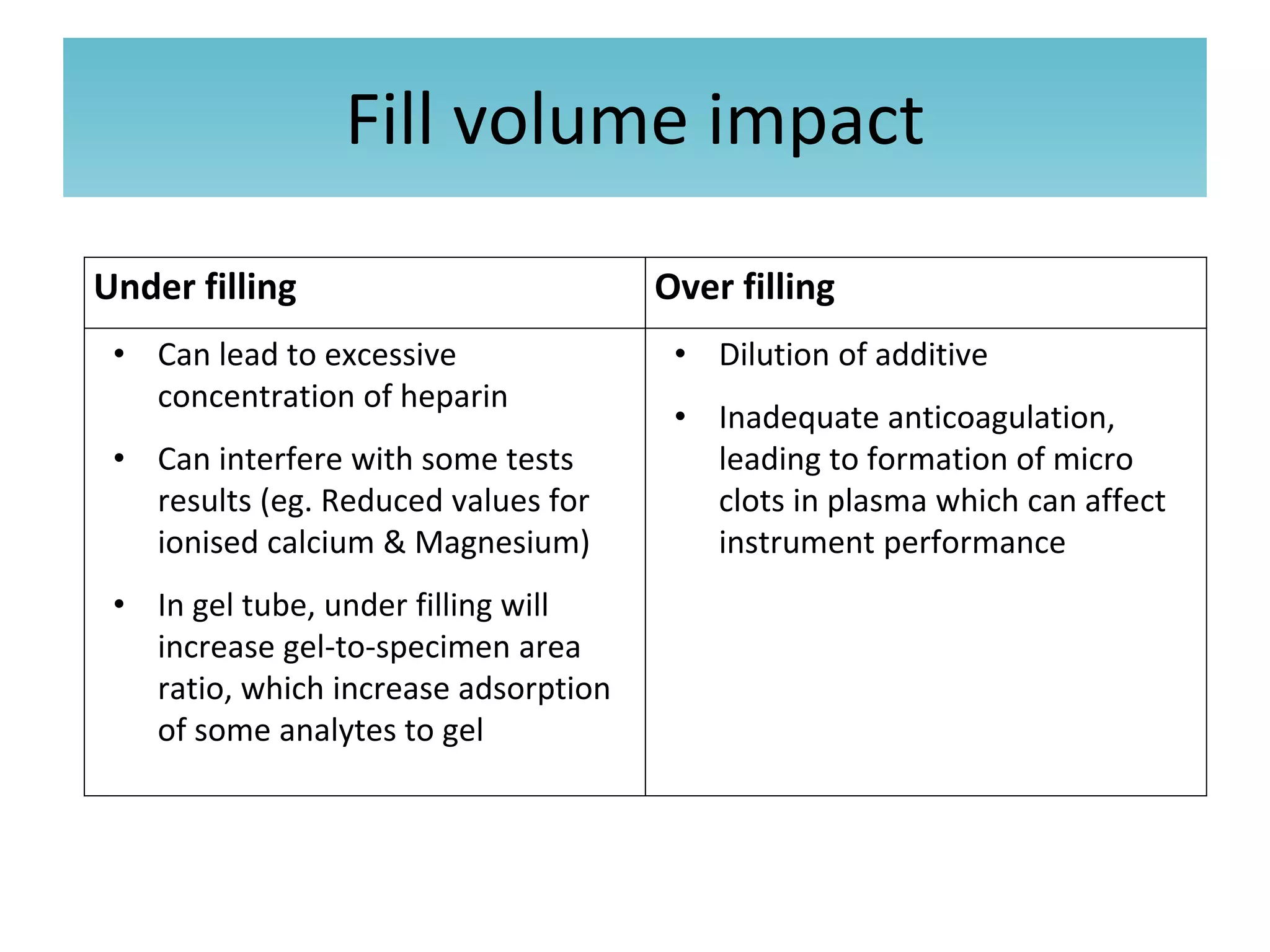
Fill volume impact
Underfilling Over filling
• Can lead to excessive
concentration of heparin
• Can interfere with some tests
results (eg. Reduced values for
ionised calcium & Magnesium)
• In gel tube, under filling will
increase gel-to-specimen area
ratio, which increase adsorption
of some analytes to gel
• Dilution of additive
• Inadequate anticoagulation,
leading to formation of micro
clots in plasma which can affect
instrument performance
33.
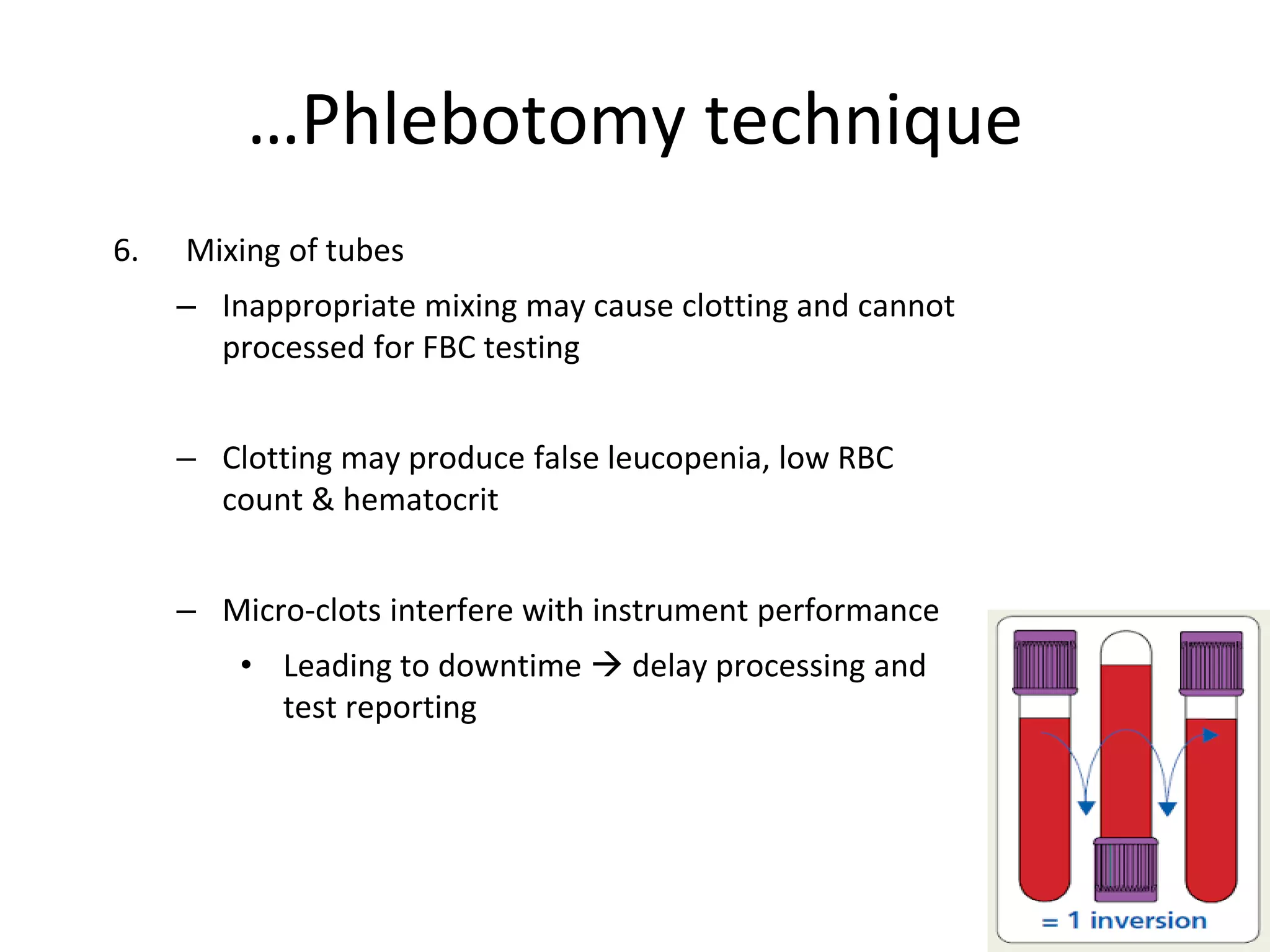
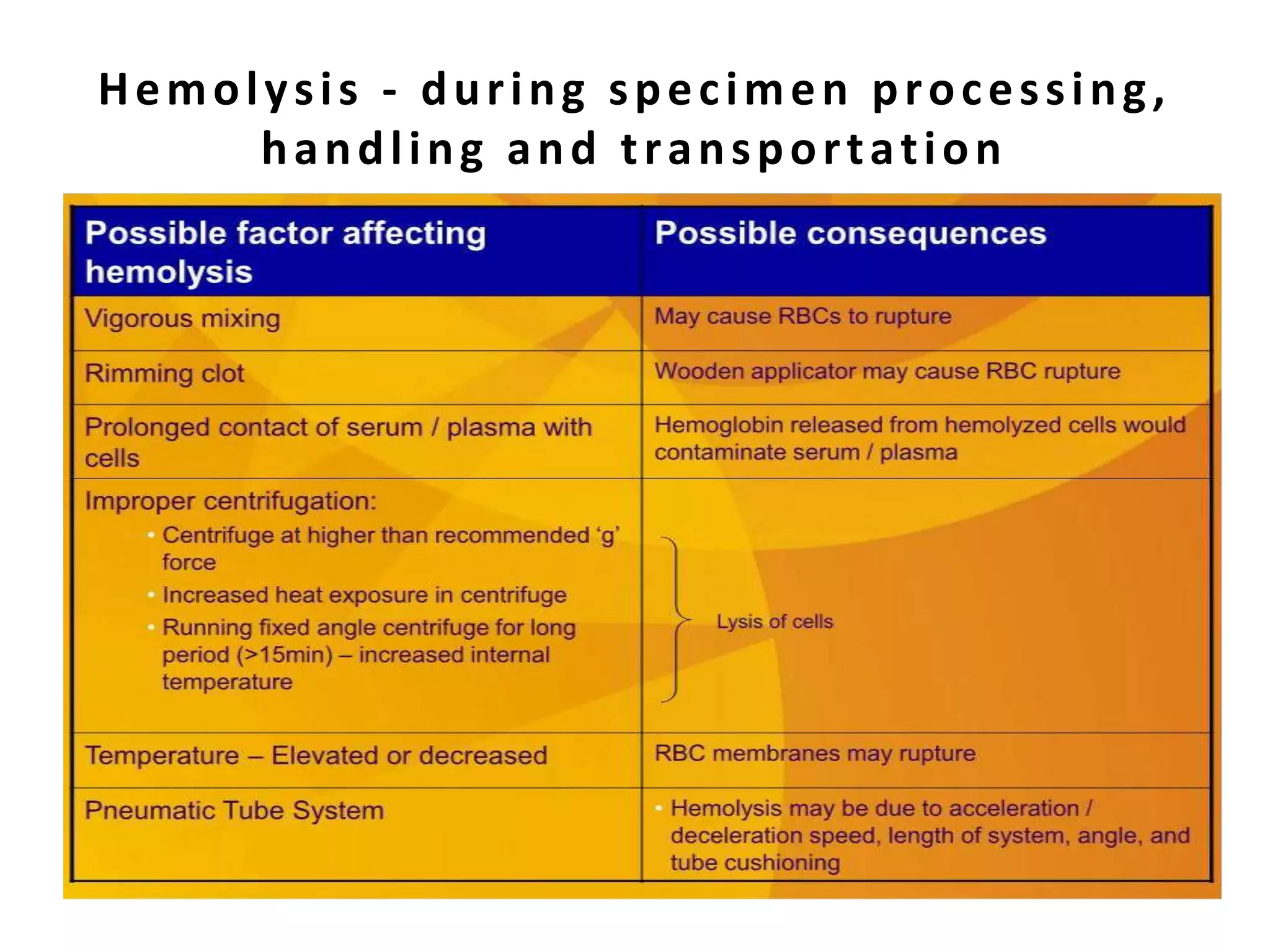
6. Mixing oftubes
– Inappropriate mixing may cause clotting and cannot
processed for FBC testing
– Clotting may produce false leucopenia, low RBC
count & hematocrit
– Micro-clots interfere with instrument performance
• Leading to downtime delay processing and
test reporting
…Phlebotomy technique
35.
• Delays of>6 hours between collection and processing
of INR or PT samples can cause significant changes in
results (i.e >10%)
• Delayed transportation to the lab affects some test
result
– E.g: K, AST, ALT etc
• Improper preservation
– e.g ice or not ACTH, ammonia, lactate etc
Sample handling
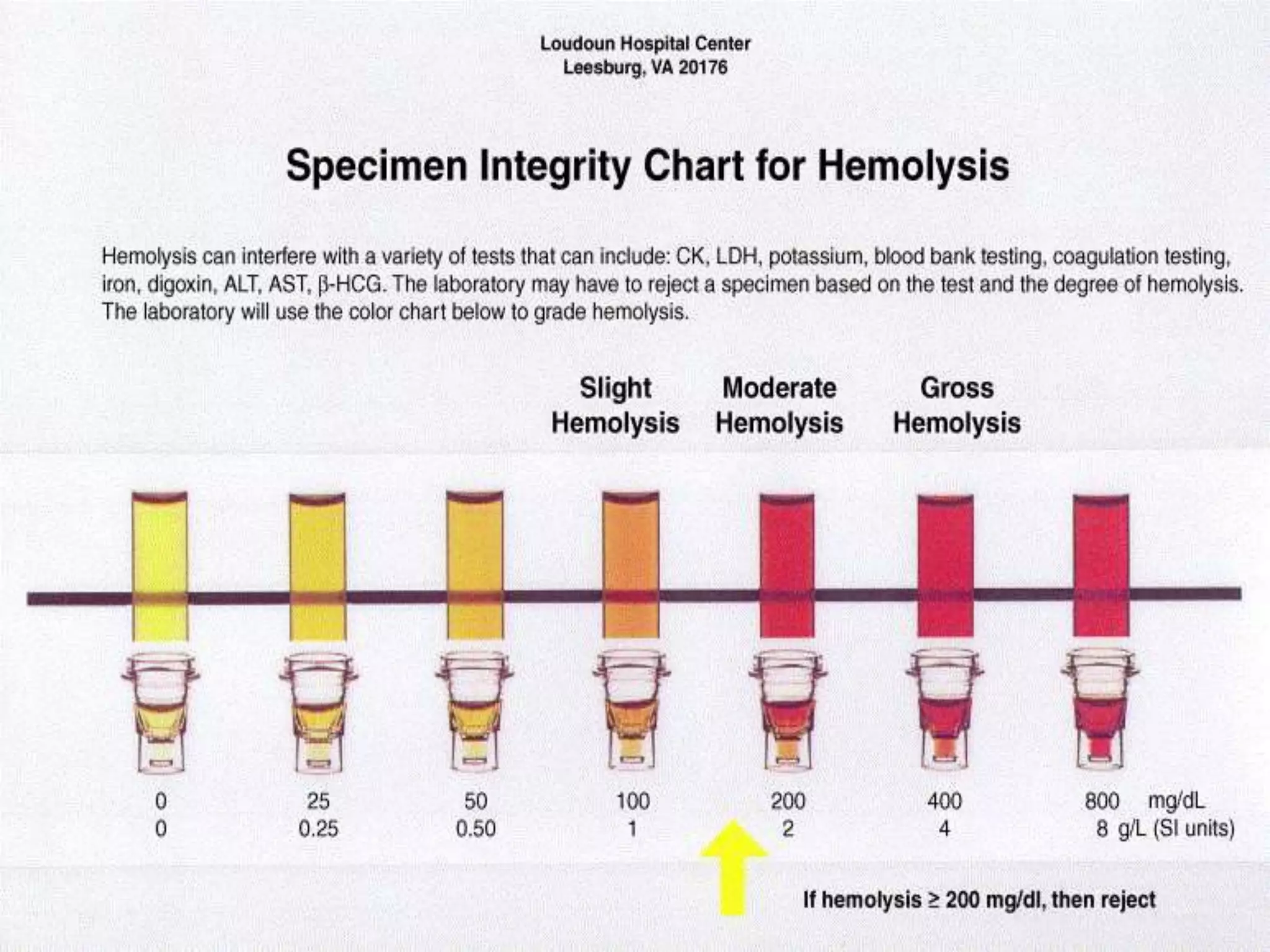
Haemolysis of sample
•Haemolysis - breakage of the RBC’s
membrane, causing release of Hb and other
internal components into the surrounding
fluid
• Test affected: K, LDH, AST, bHCG, CK,
coagulation test, iron, digoxin
• Degree of haemolysis….
39.
Haemolysis of sample
•Haemolysis can occur from two sources
– In-vivo haemolysis
• Due to pathological conditions such as AIHA or
transfusion reaction
– In-vitro haemolysis
• Can occur due to improper sample collection,
processing or transport
Reducing the causeof pre-analytical error
• Quality control
• Identify and monitor possible causes of pre-analytical errors
• QA Programs should include monitoring the sample collection
process
• Good practice
• Understand the current practice vs hospital procedures and best
practice
• Training and education programs
• Support staff by providing clear and effective training
• Tracking the cost of poor quality and errors in preanalytical procsses: proven steps labs
can use to boost patient outcomes, a lecture by Sol F. Green, BD Preanalytical Systems
43.
Ways to minimizepre-analytical errors
• Comprehensive and standardized training programs
reaching a wide range of staffs – HO, SN, MO on:
– SOP
– Specific competency assessment
– Academic seminars to inform impacts of pre-analytical errors
on patient diagnoses and and therapy
Sol F. Green “The cost of poor blood specimen quality and errors in preanalytical
processes” Clinical Biochemistry 2013
Liyun Cao Et Al. “Causes and Impact of specimen rejection in a clinical chemistry
laboratory” Clinica Chimica Acta 2016
44.
Conclusion
• Health providerrelies on laboratory test
results for management of the patients.
• The lab responsible to provide accurate and
reliable test results.
• The accuracy of test results depend greatly on
the quality of the specimens sent to the lab
45.
Take home message
•Fill up request form completely – INCLUDING DATE &
TIME of collection
• Make sure correct sample for correct pt
• Make sure correct tube container
• Make sure appropriate sample volume
• Practice correct order of draw to avoid contamination
• Any doubt, call lab for enquiry
48.
References
• Regan M,Forsman R. The impact of the laboratory on disease management, Dis Manag.
2006 Apr;9(2):122-30.
• Robert Hawkins, M.D., Managing the Pre- and Post-analytical Phases of the Total Testing
Process, Ann Lab Med 2012;32:5-16.
• Hammerling J. A., A Review of Medical Errors in Laboratory Diagnostic and Where We Are
Today, LABMEDICINE; Vol. 43, No. 2; 2012
• Sintayehu A. et al., Errors in the Total testing Process in the Clinical Chemistry Laboratory
at the University of Gondar Hospital, Euthopia J Health Sci; Vol. 28, No. 2; 2018
Editor's Notes
#5 Healthcare providers depend on accurate and precise lab results in order to do their jobs well and give patients the best possible care.
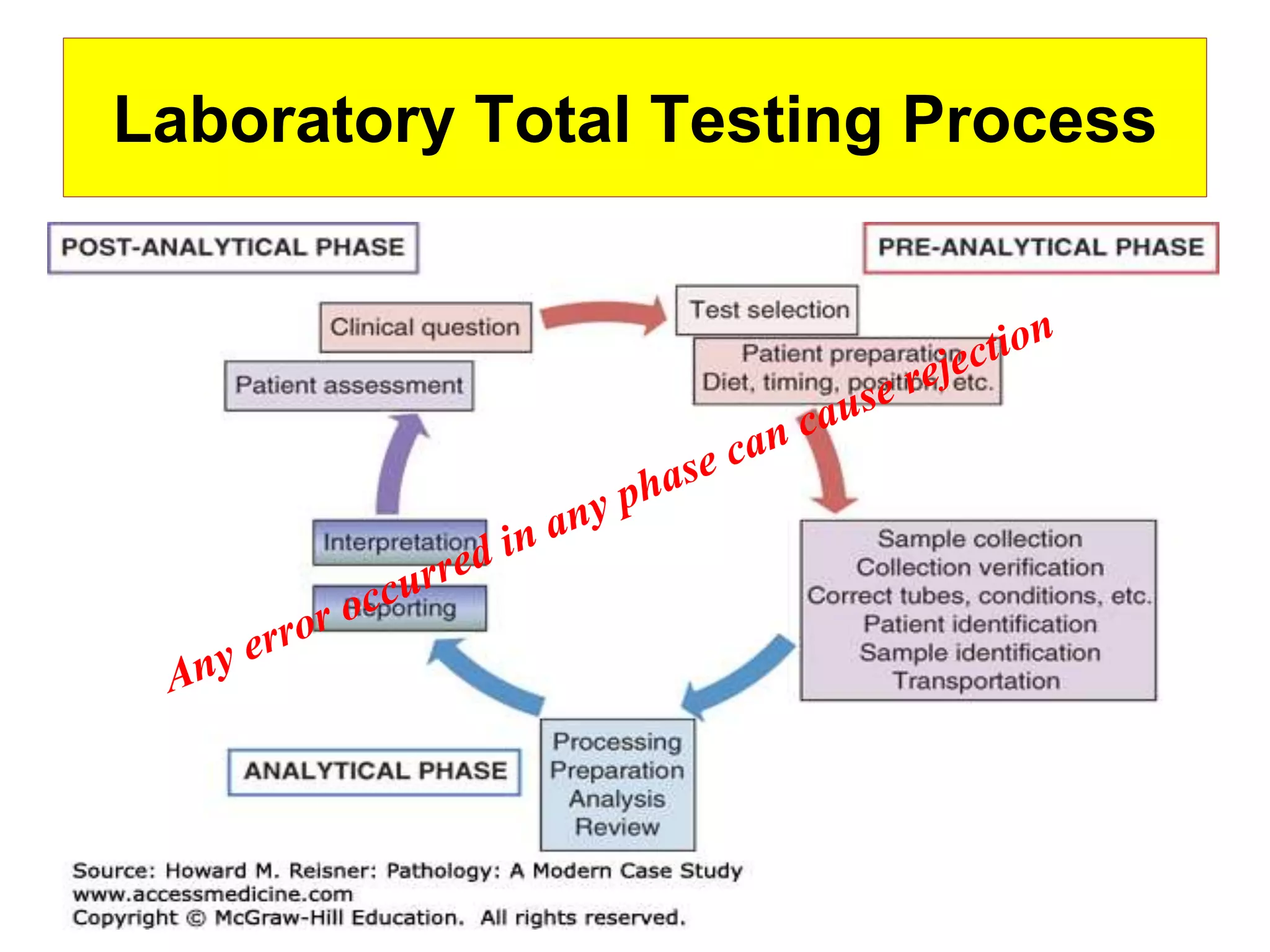
#7 Laboratory TTP is subjected to many variables as it can occur in all the phases of lab. testing
pre-ana: al steps fr time of test ordering unti; sample ready for analysis
ana: actual specimen analysis
post-ana: test reporting and interpretation