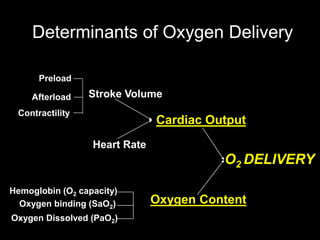
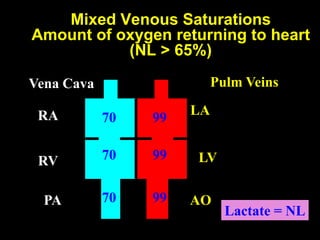
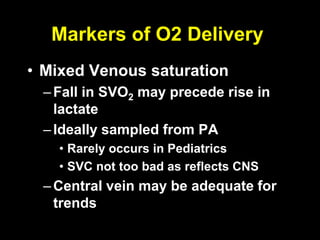
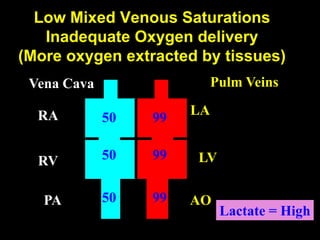
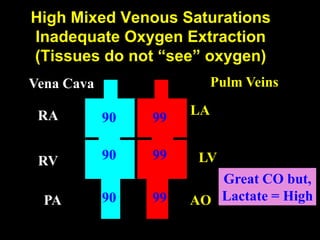
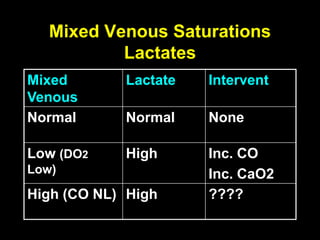
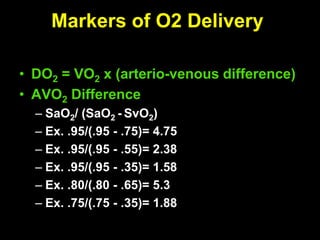
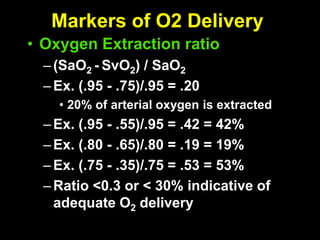
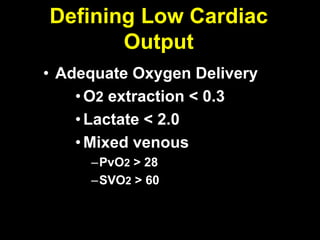
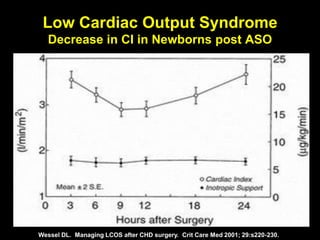
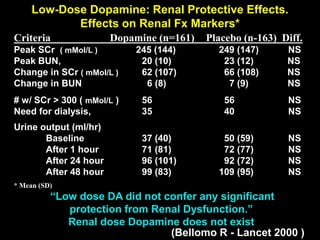
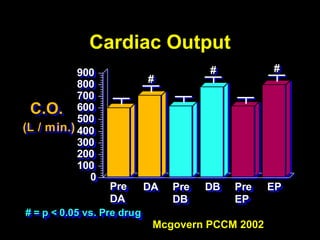
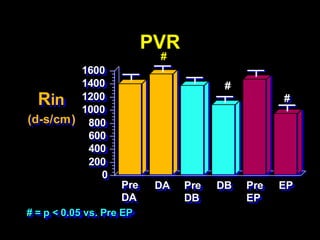
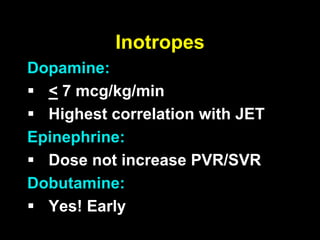

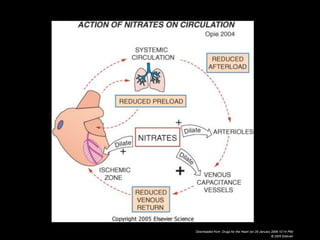

1. The document discusses various markers that can be used to define and assess low cardiac output, including lactate levels, mixed venous oxygen saturation, oxygen delivery and extraction ratio. 2. Treatment for low cardiac output syndrome focuses on improving contractility through the use of inotropic agents like calcium, dobutamine and milrinone, as well as vasodilators to reduce afterload like sodium nitroprusside. 3. The effects of various inotropes are discussed, noting that dopamine has limited benefit and epinephrine does not increase pulmonary or systemic vascular resistance like dopamine. Milrinone provides inotropic and vasodilatory effects with minimal increase in heart rate.






















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)






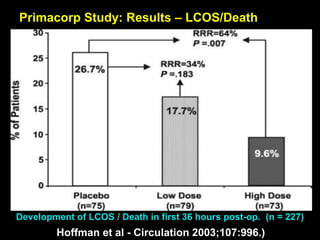
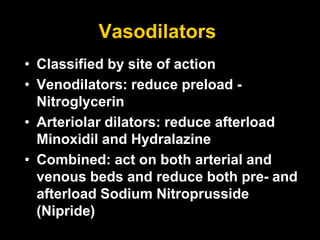
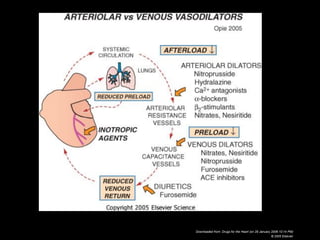
![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)



