Downloaded 35 times
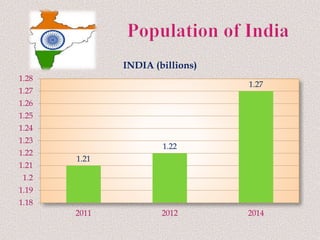
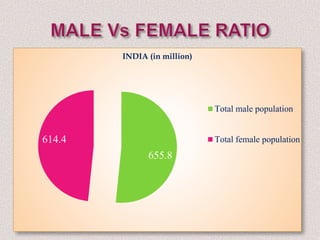
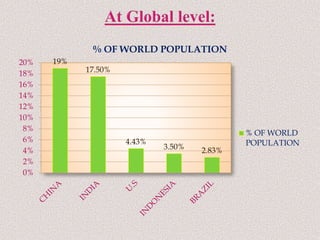





India has a population of over 1.27 billion people as of 2014, and is poised to surpass China as the world's most populated nation in the coming decades. This rapid growth strains resources and is one of India's biggest problems. The government has implemented several national population policies and family planning programs since 1951 to encourage smaller families and control population growth.






























































































