This document discusses India's national population policy and population control measures. The key points are:
- India introduced its first national population policy in 1976 which aimed to reduce population growth rates. The latest policy from 2000 aims to stabilize the population by 2045.
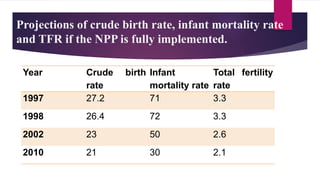
- The objectives of the 2000 policy are to address unmet needs for family planning services by 2010, achieve replacement fertility rates by 2010, and stabilize the population by 2045 in a sustainable manner.
- The policy outlines goals for 2010 like reducing infant and maternal mortality, increasing access to education and healthcare, and promoting the small family norm of two children or less. It aims to decentralize planning and use various social and economic development strategies to influence population growth