PNF : DEFINITION
Proprioceptiveneuromuscular facilitation (PNF) is a concept of treatment. Its underlying
philosophy is that all human beings, including those with disabilities, have untapped
existing potential
Proprioceptive – Having to do with any of the sensory receptors that give information
concerning movement and position of the body
Neuromuscular – Involving the nerves and the muscles
Facilitation – Making easier
3.
Basic Neurophysiological Principles
●Afterdischarge: The effect of a stimulus continues after the stimulus stops. If the
strength and duration of the stimulus increase, the afterdischarge increases as well.
The feeling of increased power that comes after a maintained static contraction is the
result of afterdischarge.
● Temporal summation: A succession of weak stimuli (subliminal) occurring
(summate) to cause excitation.
● Spatial summation: Weak stimuli applied simultaneously to different areas of the
body reinforce each other (summate) to cause excitation. Temporal and spatial
summation can combine for greater activity
4.
● Irradiation: Thisis a spreading and increased strength of a response. It occurs when
either the number of stimuli or the strength of the stimuli is increased. The response
may be either excitation or inhibition
● Successive induction: An increased excitation of the agonist muscle follows
stimulation (contraction) of their antagonists. Techniques involving reversal of
agonists, Reciprocal innervation (reciprocal inhibition), Relaxation techniques make
use of this property.
5.
BASIC PRINCIPLES OFPNF
Voss presented 11 principles of intervention at the Northwestern University Special
Therapeutic Exercise Project in 1966. These principles were developed from concepts in
the fields of neurophysiology, motor learning, and motor behaviour and are still essential
to the practice of PNF today.
• All human beings have potentials that have not been fully developed
• Normal motor development proceeds in a cervical caudal and proximodistal
direction.
• Early motor behavior is dominated by reflex activity. Mature motor behavior is
supported or reinforced by postural reflexes.
6.
• Early motorbehavior is characterized by spontaneous movement, which oscillates
between extremes of flexion and extension
• Developing motor behavior is expressed in an orderly sequence of total patterns of
movement and posture
• The growth of motor behavior has cyclic trends, as evidenced by shifts between
flexor and extensor dominance
• Normal motor development has an orderly sequence but lacks a step-by-step quality.
Overlapping of skills occurs.
• Locomotion depends on the reciprocal contraction of flexors and extensors, and
maintenance of posture requires continual adjustment for nuances of imbalance.
Antagonistic pairs of movements, reflexes, and muscles and joint motion interact as
necessary with the movement or posture.
7.
• Improvement inmotor ability is dependent on motor learning. Multisensory input
from the therapist facilitates motor learning in the client and is an integral part of the
PNF approach.
• Frequent stimulation and repetitive activity are used to promote and retain motor
learning and to develop strength and endurance.
• Goal-directed activities coupled with techniques of facilitation are used to hasten
learning of total patterns of walking and self-care activities.
8.
Diagonal Patterns
• Thediagonal patterns used in the PNF approach are the mass movement patterns
observed in most functional activities.
• Knowledge of the diagonals is necessary for identifying areas of deficiency.
9.
The Head, Neck,And Trunk patterns are referred to as
• Flexion with rotation to the right or left and
• Extension with rotation to the right or left
The UE and LE diagonals are described according to the three movement components
• Flexion and extension,
• Abduction and adduction, and
• External and internal rotation.
10.
Voss as introducedshorter descriptions for the extremity patterns in 1967 and referred to
them as :
Diagonal 1 (D1) flexion/extension and
Diagonal 2 (D2) flexion/extension
11.
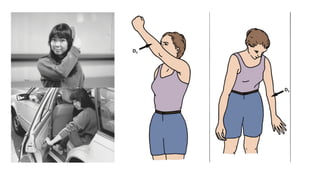
Unilateral Patterns
UE D1flexion (shoulder flexion-
adduction-external rotation):
• Scapula elevation,
• Shoulder flexion, adduction, and
external rotation;
• Elbow in flexion or extension;
• Forearm supination;
• Wrist flexion to the radial side;
• Finger flexion and adduction; and
thumb adduction
UE D1 extension (shoulder extension-
abduction-internal rotation):
• Scapula depression
• Shoulder extension, abduction, and
internal rotation;
• Elbow in flexion or extension;
forearm pronation;
• Wrist extension to the ulnar side;
• Finger extension and abduction; and
thumb in palmar abduction .
13.
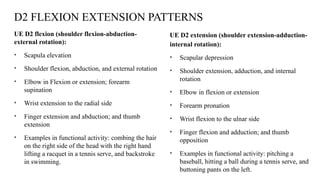
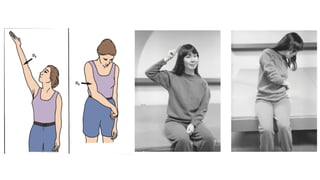
D2 FLEXION EXTENSIONPATTERNS
UE D2 flexion (shoulder flexion-abduction-
external rotation):
• Scapula elevation
• Shoulder flexion, abduction, and external rotation
• Elbow in Flexion or extension; forearm
supination
• Wrist extension to the radial side
• Finger extension and abduction; and thumb
extension
• Examples in functional activity: combing the hair
on the right side of the head with the right hand
lifting a racquet in a tennis serve, and backstroke
in swimming.
UE D2 extension (shoulder extension-adduction-
internal rotation):
• Scapular depression
• Shoulder extension, adduction, and internal
rotation
• Elbow in flexion or extension
• Forearm pronation
• Wrist flexion to the ulnar side
• Finger flexion and adduction; and thumb
opposition
• Examples in functional activity: pitching a
baseball, hitting a ball during a tennis serve, and
buttoning pants on the left.
15.
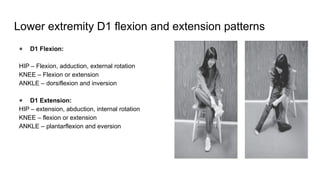
Lower extremity D1flexion and extension patterns
● D1 Flexion:
HIP – Flexion, adduction, external rotation
KNEE – Flexion or extension
ANKLE – dorsiflexion and inversion
● D1 Extension:
HIP – extension, abduction, internal rotation
KNEE – flexion or extension
ANKLE – plantarflexion and eversion
16.
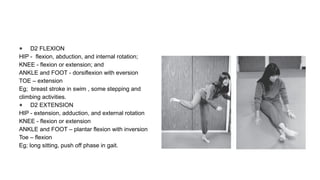
● D2 FLEXION
HIP- flexion, abduction, and internal rotation;
KNEE - flexion or extension; and
ANKLE and FOOT - dorsiflexion with eversion
TOE – extension
Eg; breast stroke in swim , some stepping and
climbing activities.
● D2 EXTENSION
HIP - extension, adduction, and external rotation
KNEE - flexion or extension
ANKLE and FOOT – plantar flexion with inversion
Toe – flexion
Eg; long sitting, push off phase in gait.
17.
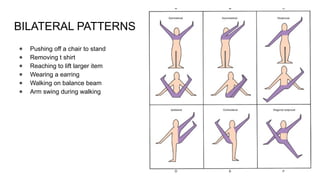
BILATERAL PATTERNS
● Pushingoff a chair to stand
● Removing t shirt
● Reaching to lift larger item
● Wearing a earring
● Walking on balance beam
● Arm swing during walking
18.
The basic proceduresfor facilitation are:
• Resistance
• Irradiation and reinforcement
• Manual contact
• Body position and body mechanics
• Auditory stimulation (commands)
• Visual stimulation
• Traction or approximation
• Quick Stretch
• Timing
• Patterns: Synergistic mass movements, components of functional normal motion
19.
Optimal Resistance
The intensityof resistance provided during an activity is dependent on the capabilities of
the patient as well as on the goal of the activity.
Resistance is used in treatment to:
• Facilitate the ability of the muscle to contract.
• Increase motor control and improve motor learning.
• Help the patient gain an awareness of motion and its direction.
• Increase strength.
• Help the patient to relax the muscle (reciprocal inhibition).
20.
Irradiation
Irradiation is definedas the spread of the response of nerve impulses of a given stimulation.
Example
• Resist muscle contractions in a sound limb to produce contraction of the muscles in the
immobilized contralateral limb.
21.
Manual Contact
The therapist’sgrip stimulates the patient’s skin receptors and other pressure receptors. This contact
gives the patient information about the proper direction of motion.
Therapeutic Goals
• Pressure on a muscle to aid that muscle’s ability to contract.
• To give the patient security and confidence.
• To promote tactile-kinesthetic perception.
• Pressure that is opposite to the direction of motion on any point of a moving limb stimulates the
synergistic limb muscles to reinforce the movement.
• Contact on the patient’s trunk to help the limb motion indirectly by promoting trunk stability.
22.
Body Position andBody Mechanics
• The therapist’s body should be in line with the desired motion or force. To line up
properly, the therapist’s shoulders and pelvis face the direction of the motion.
• The resistance comes from the therapist’s body while the hands and arms stay
comparatively relaxed. By using body weight the therapist can give prolonged
resistance without fatiguing. The relaxed hands allow the therapist to feel the
patient’s responses.
• The patient sits or lies comfortably and near the edge of the treatment table. The
therapist stands by the patient’s side,where he/she can offer the patient adequate
security and stability.
23.
Verbal Stimulation (Commands)
Theverbal command tells the patient what to do and when to do it.
The volume with which the command is given can affect the strength of the resulting
muscle contractions (Johansson et al. 1983). The therapist should give a louder command
when a strong muscle contraction is desired and use a softer and calmer tone when the
goal is relaxation or relief of pain.
The command is divided into three parts:
• Preparation: readies the patient for action
• Action: tells the patient to start the action
• Correction: tells the patient how to correct and modify the action.
24.
Visual Stimulus
Visual feedbackpromotes muscular activity,by helping with coordination, strength, and
stability.
Therapeutic goals:
• The therapist receives visual information as to whether the applied stimulus was
appropriate for the task, or whether it was too intensive or even caused pain.
• Visual input promotes a more powerful muscle contraction.
• Visual feedback helps the patient control and correct position and motion.
• Visual stimuli influence both the head and body motion.
25.
Traction and Approximation
•Traction is the elongation of the trunk or an extremity by the therapist.
• Approximation is the compression of joints.
Traction is used to:
● Promote movement pulling actions and pain relief
● Functionally – carrying heavy object, pulling a door
● Contraindications – acute post operative ststus, recent fractures.
26.
• Approximation isused to:
Facilitate joint receptors responsible for stability and
promotes postural control, proximal stability.
Can be subtitued with weighted vest and functional weight bearing activites in home
programes
• There are three ways to apply the approximation:
o Quick approximation: the force is applied quickly to elicit a reflex-type
response.
o Slow approximation: the force is applied gradually up to the patient’s tolerance.
o Maintained approximation: After either a quick or slow approximation, the
pressure will be maintained as long as necessary for the muscles to build up the
proper muscle tension.
27.
Timing
Timing is thesequence of movements
In adults, normal timing of most coordinated and efficient motions is from distal to
proximal.
Sequencing: Movement typically proceeds from the distal parts (e.g., fingers, toes) toward
the proximal parts (e.g., trunk, shoulder).Example: A therapist guides a patient in a PNF
pattern for reaching, focusing on a smooth motion where the fingers and hand move first,
followed by the wrist, elbow, and finally the shoulder, in a continuous flow.
Timing for emphasis involves changing the normal sequencing of motions to emphasize a
particular muscle or a desired activity.
28.
PNF TECHNIQUES
PNF techniquesare divided into three categories:
• Directed to the Agonists
• Reversal of the Antagonists
• Promoting Relaxation
29.
Techniques Directed tothe Agonists : Repeated Contractions
• Repeated Contractions
• Repetition of an activity builds strength, ROM, endurance, and helps in motor learning.
• Example: Repeated shoulder flexion with resistance to improve strength.
31.
Rhythmic Initiation
• Toimprove the ability to initiate movement and reduce rigidity.
• Movement is facilitates in series of ROM
• Passive ROM — Active assisted ROM — Active ROM — Movement with resistance
33.
Techniques Involving Reversalof Antagonists
• Slow Reversal : Isotonic contraction of antagonist followed by isotonic contraction of
agonist without relaxation.
• To promote coordination and control of movement between agonist and antagonist.
• Patient performs resisted shoulder extension first, then smoothly reverses to shoulder
flexion against resistance without pause.
35.
Slow Reversal Hold
•Same as slow reversal but ends with an isometric hold at the end of the movement.
• Slow Reversal Hold for Shoulder Flexion: Patient performs resisted shoulder extension,
then reverses to flexion against resistance and holds the end position isometrically.
37.
Stabilizing Reversals
• Alternatingisotonic contractions opposed by enough resistance to prevent motion.
The command is a dynamic command (push against my hands or don’t let me push
you) and the therapist allows only a very small movement.
• To develop stability and postural control.
• Maintaining upright sitting against alternating manual resistance.
38.
Rhythmic Stabilization
Alternating isometriccontractions against resistance, no motion intended.
Examples
• Patient is standing on one leg for balance training.
• Therapist places hands on the patient’s pelvis from front and back.
• Therapist applies gentle simultaneous pushes in both directions.
• Patient activates hip and trunk muscles to maintain posture without moving.
40.
Relaxation Techniques
Contract–Relax :Resisted isotonic contraction of the restricting muscles (antagonists)
followed by relaxation and movement into the new increased range.
Example :
• Patient lies supine with the arm extended (elbow near full extension).
• Therapist passively moves the elbow into flexion until resistance or tightness is felt.
• Patient performs an isotonic contraction of the antagonist (elbow extensors — triceps)
against maximal resistance for 5–10 seconds.
• Patient relaxes, and therapist passively moves the elbow further into flexion.
• Repeat 3–5 times until maximal flexion is achieved.
42.
Hold relax
Hold-relax isperformed in the same sequence as contract relax but involves an isometric
contraction (no movement allowed) of the antagonist, followed by relaxation and then
active movement into the agonistic pattern.
It has been recommended that the static contraction be held for 3 seconds to achieve the
greatest improvement in ROM.
Because this technique involves an isometric contraction against resistance, it is
particularly beneficial in a client with pain or acute orthopedic conditions.
44.
Rhythmic rotation
Rhythmic rotationis effective in decreasing spasticity and increasing ROM. The therapist
passively moves the body part in the desired pattern.
When tightness or restriction of movement is felt, the therapist rotates the body part
Slowly and rhythmically in both directions.
After relaxation is felt, the therapist continues to move the body part into the newly
available range.
46.
Proprioceptive Neuromuscular FacilitationExercices versus Lumbar Stabilization
Exercises for Chronic Low Back Pain Patients: A Randomized Interventional Study
Research design:
● A prospective, comparative, randomized interventional study
Sampling technique:
● Twenty two patients were selected and divided into two groups
‑
Sample population:
● Patients with mechanical low back pain of more than 3 months, in both males and
females, of age 20–45 years.
Duration of intervention :
● Both group received 3 treatment sessions per week for 4 weeks, each session lasting
for 45 min.
47.
Inclusion criteria :
●Participants aged 20–45 years.
● Diagnosis: Individuals with mechanical low back pain lasting more than 3 months.
Exclusion criteria
● Patients having the systemic illness, central or peripheral neurologic signs and
specific causes of low back pain such as disc herniation, lumbar stenosis, spinal
deformity, fractures, and spondylolisthesis were excluded.
● Patients having systemic illness (tumor and rheumatologic disease) and psychiatric
illness were also excluded from the study
Tools used
● Visual Analog Scale (VAS), modified Schober’s test, Modified Oswestry Low Back
Pain Disability Questionnaire (ODI), Roland and Morris Low Back Pain and
Disability Questionnaire (RMDQ).
48.
Intervention protocol :
●Patients in the PNF Group received concentric and eccentric contractions of agonist
and antagonist muscles, patterns such as chopping, lifting, bilateral leg, and trunk
lateral flexion. LSE Group received core strengthening exercises
Result
● PNF group showed significant improvement in pain on VAS (P = 0.003; 95%
confidence interval [CI[, 2.15–3.01), in disability on ODI (P = 0.001, 95% CI, 12.09–
20.1), and in lumbar flexibility Modified Schober’s test (P = 0.000, 95% CI, 5.15–
5.93) On RMDQ, there was no statistically significant difference between PNF and
LSE groups (P = 0.061, 95% CI, 6.87–8.97).
49.
Comparison of TaskOriented Approach Versus Proprioceptive Neuromuscular
Facilitation Technique on Functional Ambulation in Stroke Patients
Research design :
● Single centre randomized control trial.
Sampling technique :
● Convenient sampling with random assignment
Sample population :
● A total of 30 stroke patients.
Duration of intervention :
● Each protocol given 45minutes per session 5 days a week for two months.
Inclusion criteria
● Population all stroke survivors: Male and female both.
● Types of stroke -Ischemic or hemorrhagic.
● No more than one stroke episode.
● Can walk at least one minute without support.
● No incidence of any other significant neurological disorder.
● Ability to communicate verbally.
50.
Exclusion criteria
● Seizuredisorder.
● Primary hearing impairment and Severe visual impairment.
● An orthopedic condition affecting their natural gait.
● Any other significant neurological or orthopedic disorders of gait including
amputation
Tools used
● Functional gait assessment scale
Intervention protocol
Result
51.
Intervention protocol:
PNF: Lowerextremity
Flexion-abduction-external rotation (knee flexed and knee extended)
Extension-adduction-internal rotation (knee flexed and knee extended)
Flexion-adduction-internal rotation (knee flexed and knee extended)
Extension-abduction-external rotation (knee flexed and knee extended).
Upper extremity:
Flexion-abduction-external rotation (elbow flexed and elbow extended).
Extension-adduction-internal rotation (elbow flexed and elbow extended).
Flexion-adduction-internal rotation (elbow flexed and elbow extended).
Extension-abduction-external rotation (elbow flexed and elbow extended)
52.
TASK ORIENTED APPROACH
●Reaching towards objects across table while standing with symmetrical weight
distribution over both legs.
● Walking over the balance beam.
● Forward walking
● Backward walking.
● Sideway walking.
● Obstacle Crossing
● Bending and picking up objects from the floor.
● Walking in real life situation like uneven surfaces and narrow spaces.
● Stair climbing.
● Walking in a ramp.
53.
Results:
● From thestatistical result of this study, it is seen that there is no significance
difference in FGA scale between two groups. This data suggests that TOA and PNF
approaches are equally efficacious in treating functional ambulation in stroke patients
and there is a significant improvement within the two experimental group.
54.
Effectiveness of ProprioceptiveNeuromuscular Facilitation as an Adjunct to
Conventional Therapy in Conservatively Managed Distal Radius Fractures: A
Randomized Controlled Trial
Research design :
● A Randomized Controlled Trial
Study setting:
Sampling technique :
● Simple random sampling using lottery method.
Sample population :
● 60 subjects diagnosed with distal radius fracture.
● The subjects were randomly assigned into 2 groups by lottery method
Duration of intervention:
● 12 weeks
● Follow up evaluation was done at the end of 2nd week, 6th and 12th week and documented for both the
groups.
55.
Inclusion criteria
Patients inthe age group 20 to 60 years of either gender, radiologically diagnosed distal
radius fracture, reporting to the physiotherapy department after immobilization and cast
removal were included in this study
Exclusion criteria
Other ipsilateral upper limb fractures, neurovascular deficits, Sudeck’s Dystrophy.
Informed consent was taken and subjects were explained about the intervention they
were going to be given.
Tools used
Numerical rating pain scale (NRPS), range of motion (ROM), Patient-Rated Wrist
Evaluation Questionnaire (PRWE), Disabilities of the Arm, Shoulder and Hand
Questionnaire (DASH).
56.
Intervention protocol
Group B– conventional therapy
● Participants received Maitland’s passive mobilizations, initially grade I oscillations
dorsal glide for increase in flexion, volar glide for increase in extension and dorsal
glide for increase in supination, volar glide for increase in pronation at proximal and
distal radio ulnar joint and cryotherapy for 15 minutes, followed by home exercises.
● Home Exercises Program: Active assisted and isometric exercise range of motion of
wrist, supination and pronation activities, grip strengthening and intrinsic muscle
strengthening were taught to the patients as home exercise program for each group.
57.
GroupA -Proprioceptive NeuromuscularFacilitation + Conventional therapy
● Maitland’s mobilization followed by PNF techniques such as rhythmic initiation,
combinations of isotonic, dynamic reversals, stabilizing reversals rhythmic
stabilization, repeater stretch, hold relax and contract relax were tailored to
individual needs of the patient, followed by home exercise program
Conclusion
● This study concludes that there were significant improvement seen in both the groups
in NPRS, ROM, PRWE, DASH but the experimental group treated with PNF along
with conventional therapy showed better results than control group treated with
conventional therapy alone.
58.
Reference
● Adler, S.S., Beckers, D., & Buck, M. (2014). PNF in practice: An illustrated guide
(4th ed.). Springer.
● Early, M. B., & Atchison, B. (2018). Pedretti’s occupational therapy: Practice skills
for physical dysfunction (8th ed.). Elsevier.
59.
● Research design
●Study setting
● Sampling technique
● Sample population
● Duration of intervention
● Variables
● Duration of intervention
● Inclusion criteria
● Exclusion criteria
● Tools used
● Intervention protocol
● Result