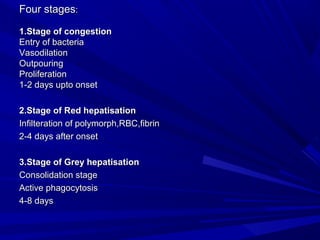
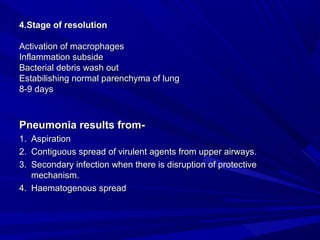
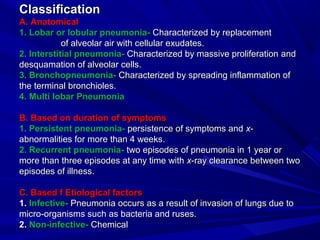
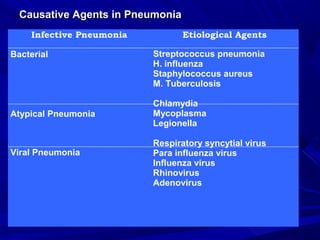
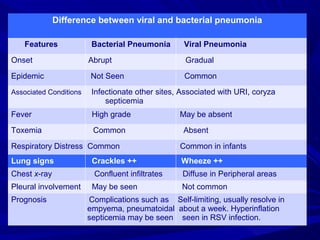
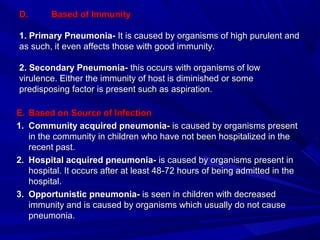
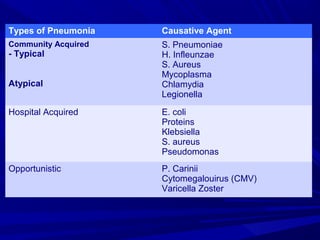
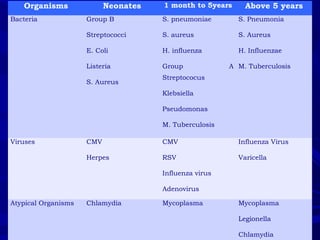
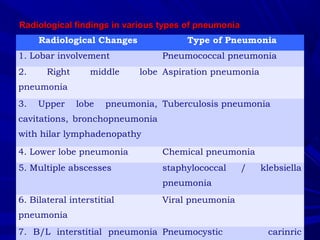
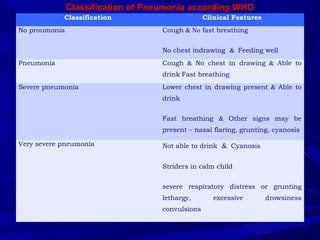
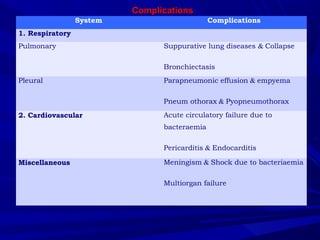
This document discusses pneumonia, including its pathogenesis, stages, classification, causative agents, and pre-disposing factors. Pneumonia is an inflammatory process of the lung parenchyma that is usually caused by bacteria, viruses, or other microorganisms entering the lungs. It affects the small air sacs (alveoli) of the lungs and can cause symptoms like cough, fever, and difficulty breathing. The document outlines the four stages of pneumonia and provides details on the various types based on location, duration, etiology, immunity, and source of infection. Common causative organisms are also identified based on patient age and immune status. Pre-disposing factors that increase risk include young age, preexisting lung conditions,
![ fpfdRlkn'kZ esa ia- jkts'oj nÙk 'kkL=h us blsfpfdRlkn'kZ esa ia- jkts'oj nÙk 'kkL=h us bls
okr&'ys"eksYc.k lfÂikr Toj ;k 'olud Toj dh laKk nh gSAokr&'ys"eksYc.k lfÂikr Toj ;k 'olud Toj dh laKk nh gSA
ckyxzgksa esa fir`xzg ds y{k.kksa dk vR;f/d lkeatL;ckyxzgksa esa fir`xzg ds y{k.kksa dk vR;f/d lkeatL;
U;qeksfu;k ds y{k.kksa ls feyrk gSA ;fn le; ij mfpr mipkj uU;qeksfu;k ds y{k.kksa ls feyrk gSA ;fn le; ij mfpr mipkj u
fd;k tk; rks 'kS'koh; e`R;q dk dkj.k Hkh curk gSAfd;k tk; rks 'kS'koh; e`R;q dk dkj.k Hkh curk gSA
okr'ys"eksYc.k lfuikr Toj esa ia- jkts'oj nÙk 'kkL=kh th usokr'ys"eksYc.k lfuikr Toj esa ia- jkts'oj nÙk 'kkL=kh th us
fuEu fpfdRlk dgh g kfuEu fpfdRlk dgh g k
1- f=HkqoudhfrZ] J`axjkHkz J`axHkLe] 'k)q ujlkj ,oa jlflUnwj1- f=HkqoudhfrZ] J`axjkHkz J`axHkLe] 'k)q ujlkj ,oa jlflUnwj
dk ;ksx o;kuqlkj cukdj fnu esa 6 ckj iku] lsagq.Mi=&Lojldk ;ksx o;kuqlkj cukdj fnu esa 6 ckj iku] lsagq.Mi=&Lojl
rFkk e/qk ls nsaArFkk e/qk ls nsaA
2-2- 'oklÑPNª gksus ij lkSHkkX; oVh] 'okldklfpUrkef.k]'oklÑPNª gksus ij lkSHkkX; oVh] 'okldklfpUrkef.k]
eYypUnzksn; J`axHkLe dk ;ksx fnu esa 6 ckjeYypUnzksn; J`axHkLe dk ;ksx fnu esa 6 ckj
dkdM+kJ`axh ,oa eqysBh pw.kZ ls rFkk e/qk ls nsaAdkdM+kJ`axh ,oa eqysBh pw.kZ ls rFkk e/qk ls nsaA
3-3- dSjkrkfn DokFk dk iz;ksx djsaAdSjkrkfn DokFk dk iz;ksx djsaA
4-4- fiIiY;fn pw.kZ ¼;ks-j-½ Vad.kkfn ;ksx ¼fl-Hks-e-ek-½]fiIiY;fn pw.kZ ¼;ks-j-½ Vad.kkfn ;ksx ¼fl-Hks-e-ek-½]
fgaXkqykfn oVh dk iz;ksx mRQqfYydk esa fd;k tk;AfgaXkqykfn oVh dk iz;ksx mRQqfYydk esa fd;k tk;A](https://image.slidesharecdn.com/pneumoniapptbymukhtaralam-151230141723/85/Pneumonia-28-320.jpg)
![mYQqfYydk dh 'kkL=kh; fpfdRlkmYQqfYydk dh 'kkL=kh; fpfdRlk
f'k'kq dh fpfdRlkf'k'kq dh fpfdRlk
^fu% lkj;sTtykSdkHkh jDra p tBjkÙknk*^fu% lkj;sTtykSdkHkh jDra p tBjkÙknk*
1 f'k'kq ds mnj esa tykSdk yxkdj jDreks{k.k djsaA1 f'k'kq ds mnj esa tykSdk yxkdj jDreks{k.k djsaA
2 ckyd ds mnj ij vfXu ls Losnu djsaA2 ckyd ds mnj ij vfXu ls Losnu djsaA (hast sweda upto 6(hast sweda upto 6
months)months)
ekrk dh fpfdRlkekrk dh fpfdRlk
11 LrU; 'kks/kuLrU; 'kks/ku
ddksZV] 'kq.Bh] eqLrk] dadksy ,oa vfrfo"kk leHkkx ysdjddksZV] 'kq.Bh] eqLrk] dadksy ,oa vfrfo"kk leHkkx ysdj
pw.kZ dj nw/k ds vuqiku ls ekrk ;k ?kk=h dks fiykdj nw/kpw.kZ dj nw/k ds vuqiku ls ekrk ;k ?kk=h dks fiykdj nw/k
dks 'kq) dj nsaAdks 'kq) dj nsaA
vfXuuk Losn;s}kvfXuuk Losn;s}kvvfi nkg;sPp 'kykd;kAfi nkg;sPp 'kykd;kA
tBsj fcUnqdkdkja i`"BHkkxs ;Fkk /qzoea~AAtBsj fcUnqdkdkja i`"BHkkxs ;Fkk /qzoea~AA
2 ckyd ds mnj ij vfXu ls Losnu djsa ;k mnj ij vkSj ihB ij2 ckyd ds mnj ij vfXu ls Losnu djsa ;k mnj ij vkSj ihB ij
'kykdk dj fcUnq ds vkdkj dk nkg djsaA'kykdk dj fcUnq ds vkdkj dk nkg djsaA](https://image.slidesharecdn.com/pneumoniapptbymukhtaralam-151230141723/85/Pneumonia-29-320.jpg)
![vkH;Urj iz;qDr vkS"kf/k;k¡vkH;Urj iz;qDr vkS"kf/k;k¡
1-1- fcYoewykfn DokFkfcYoewykfn DokFk
fcYoewyda uhjnks o`dh f=Qyka rFkkfcYoewyda uhjnks o`dh f=Qyka rFkk
flafgdk};e~flafgdk};e~
xkSMfefJra DofFkra lea ik;sfPN'kqaxkSMfefJra DofFkra lea ik;sfPN'kqa
QqfYydkige~AAQqfYydkige~AA
fcYoewykfn DokFk& fcYoewy] eqLrk] ikBk] f=QykfcYoewykfn DokFk& fcYoewy] eqLrk] ikBk] f=Qyk
rFkk dVsjh}; leHkkx dk DokFk cukdj leHkkx xqM+rFkk dVsjh}; leHkkx dk DokFk cukdj leHkkx xqM+
dk e| feykdj f'k'kq dks ;Fkkek=k fiykus ls QqfYydkdk e| feykdj f'k'kq dks ;Fkkek=k fiykus ls QqfYydk
O;kf/k Bhd gksrh gSaAO;kf/k Bhd gksrh gSaA
2-2- fiIiY;kfn pw.kZfiIiY;kfn pw.kZ
fiIiyh] fiIiyhewy] xtfiIiyh] 'kq.Bh] =k;ek.k] nk:gfjnzk]fiIiyh] fiIiyhewy] xtfiIiyh] 'kq.Bh] =k;ek.k] nk:gfjnzk]
HkkxõhZ] yox ] 'kq-Vad.k] ?k`rdqekjh] gjhrdh oHkkxõhZ] yox ] 'kq-Vad.k] ?k`rdqekjh] gjhrdh o](https://image.slidesharecdn.com/pneumoniapptbymukhtaralam-151230141723/85/Pneumonia-30-320.jpg)