Download to read offline
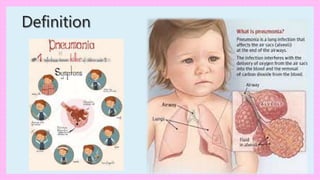
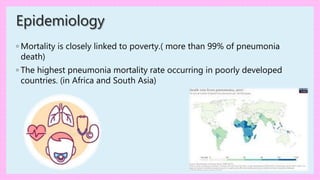
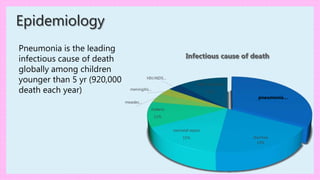





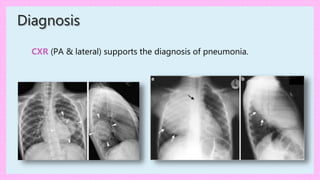






Pneumonia is an inflammation of the lung parenchyma that is most commonly caused by infectious agents like bacteria and viruses. It is a leading cause of death among children under 5 years old globally. Symptoms include cough, fever, tachypnea, and respiratory distress. Diagnosis involves physical exam findings and chest x-ray. Treatment depends on the suspected cause and severity of illness, and may involve hospitalization, antibiotics, oxygen support, and fluid resuscitation. Prognosis is generally good with appropriate treatment, but complications can occur.



































































