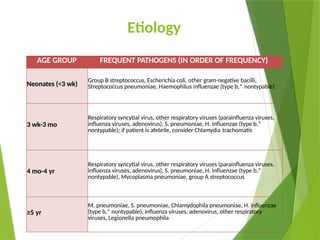
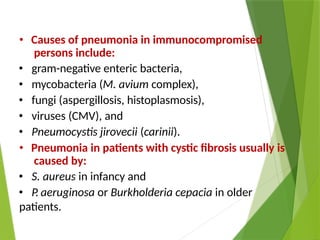
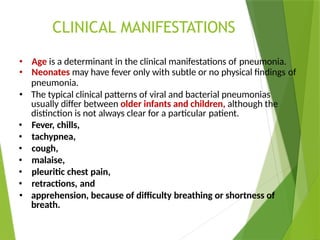
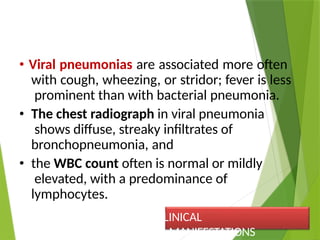
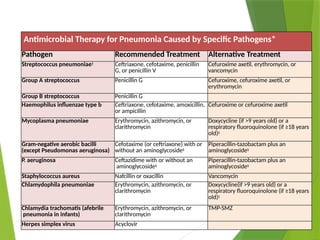
Pneumonia is a lower respiratory tract infection characterized by inflammation and consolidation in the alveolar spaces, with various types including lobar pneumonia and bronchopneumonia. The condition has significant morbidity and mortality rates in children, particularly in developing countries, and can arise from infectious and non-infectious causes. Clinical manifestations, diagnosis, and treatment strategies vary based on age, severity, and the suspected pathogens, with empirical antibiotic therapy being a common approach for community-acquired cases.