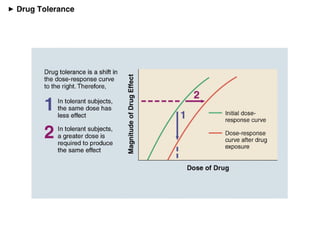
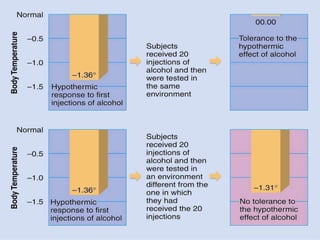
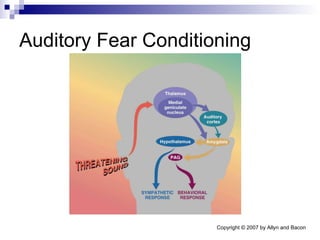
Health psychology focuses on how psychological factors impact physical health. Addiction involves tolerance, dependence, and continued use despite consequences. The brain's dopamine system is involved in addiction, signaling reward and craving. Chronic stress can impair immune function and increase disease risk by activating stress responses. Emotions involve the amygdala and other brain regions, and fear conditioning demonstrates the amygdala's role in processing fearful stimuli.





















































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)
















