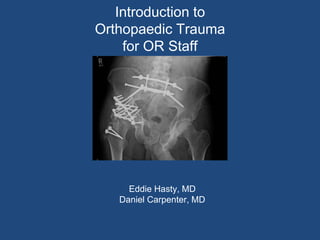
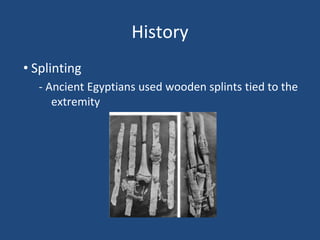
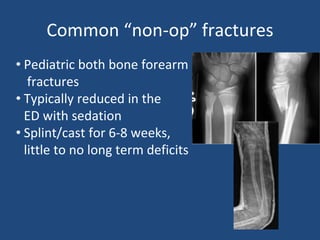
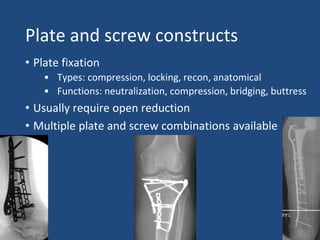
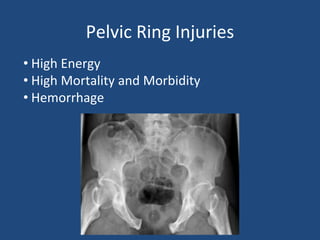
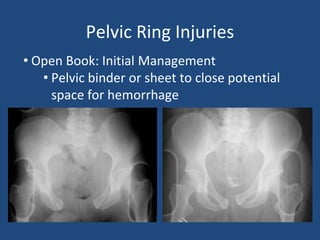
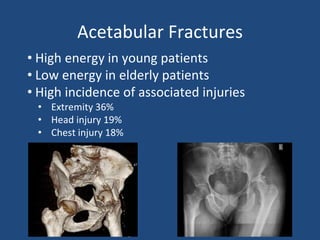
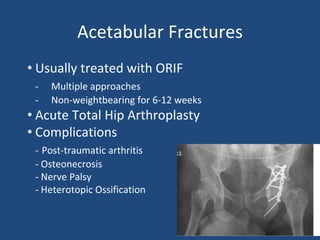
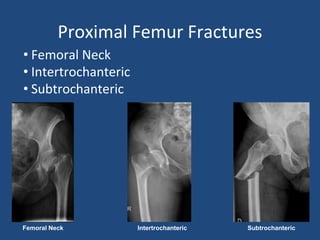
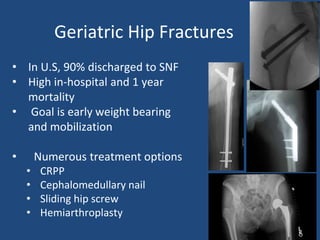
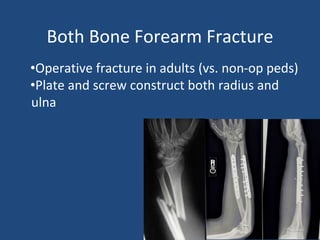
This document provides an introduction to orthopaedic trauma for operating room staff. It discusses the history of orthopaedic trauma treatment including splinting and traction. Common traumatic injuries like pelvic fractures, acetabular fractures, and femoral fractures are reviewed along with typical treatment approaches like external and internal fixation. Non-operative treatment with casting is compared to operative fixation options. The principles of damage control surgery are introduced. Common fracture patterns are summarized along with associated operative procedures and goals of treatment.