Downloaded 447 times












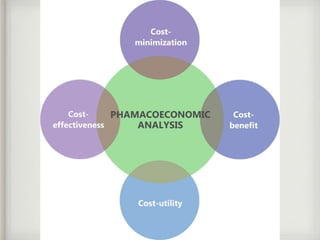










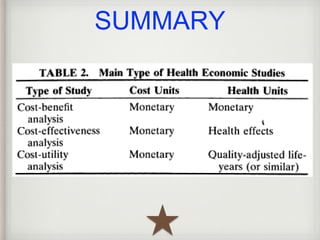






This document provides an overview of pharmacoeconomics. It discusses the history and basics, including definitions of key terms like QALY. Methods of pharmacoeconomic evaluation are outlined, including cost-minimization analysis, cost-effectiveness analysis, cost-utility analysis, and cost-benefit analysis. Challenges in pharmacoeconomic evaluations are also summarized, such as the need for training and standardization of methods.