This document provides an introduction to pharmacoeconomics including:
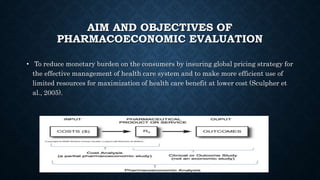
- Pharmacoeconomics compares the costs and benefits of pharmaceutical products and services to help optimize the allocation of healthcare resources.
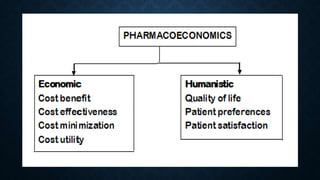
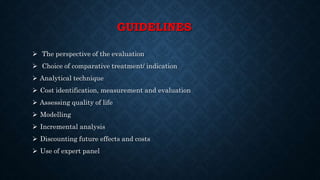
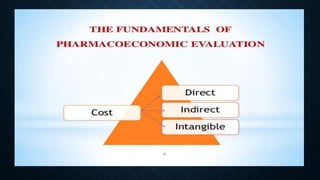
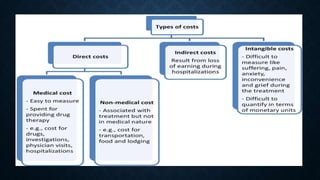
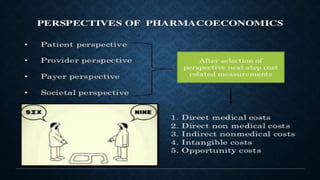
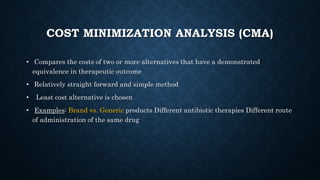
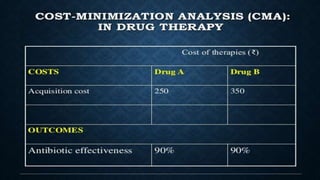
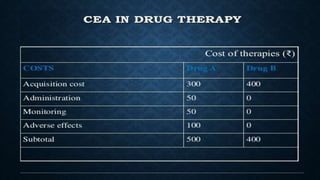
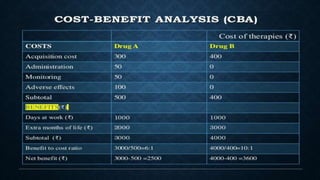
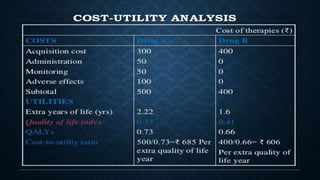
- It evaluates the costs of drug therapy from different perspectives (e.g. patient, provider, payer) and uses various analytical techniques (e.g. cost-minimization analysis, cost-effectiveness analysis, cost-benefit analysis).
- Pharmacoeconomic evaluations are important for clinical and policy decision making to improve health outcomes given limited healthcare budgets.