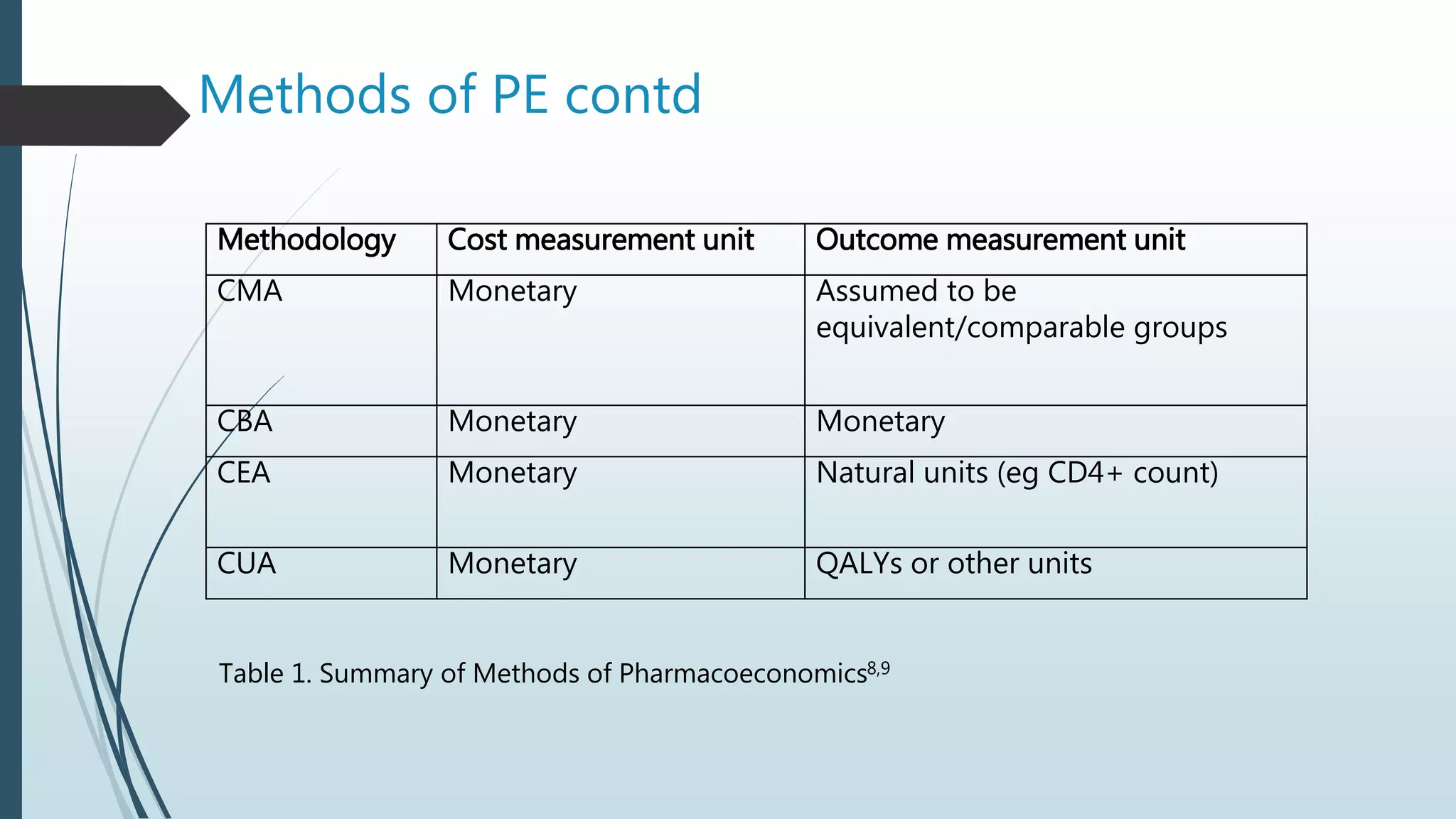
This document defines pharmacoeconomics and outlines its key principles and methods. Pharmacoeconomics is defined as the description and analysis of the costs of drug therapy to health systems and society. It considers the economic relationships of drug research, production, distribution, and use. Methods of pharmacoeconomics include cost-of-illness analysis, cost-benefit analysis, cost-effectiveness analysis, and cost-utility analysis. These methods are used to evaluate healthcare programs and therapies to determine the optimal use of resources. Pharmacoeconomics can help inform decisions around drug formularies, new drug approvals, and pharmaceutical policies.