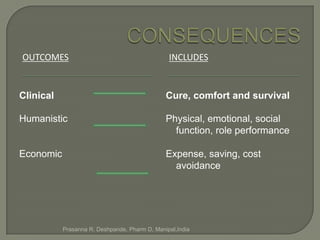
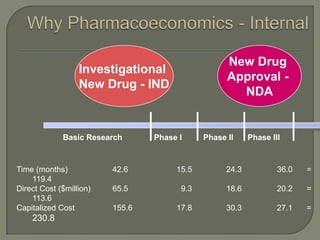
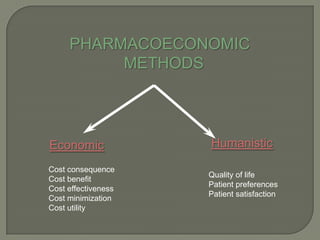
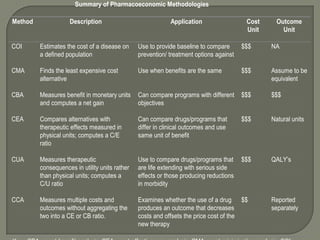
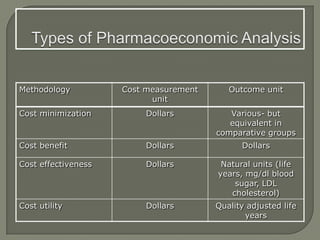
Pharmacoeconomics is the description and analysis of the costs of drug therapy to health systems and society. It identifies, measures, and compares the costs and outcomes of drug therapies and healthcare programs. Key methods include cost-of-illness, cost-benefit analysis, cost-effectiveness analysis, and cost-utility analysis. These evaluate the economic, clinical, and humanistic impacts of healthcare interventions from various perspectives including patients, providers, payers, and society.