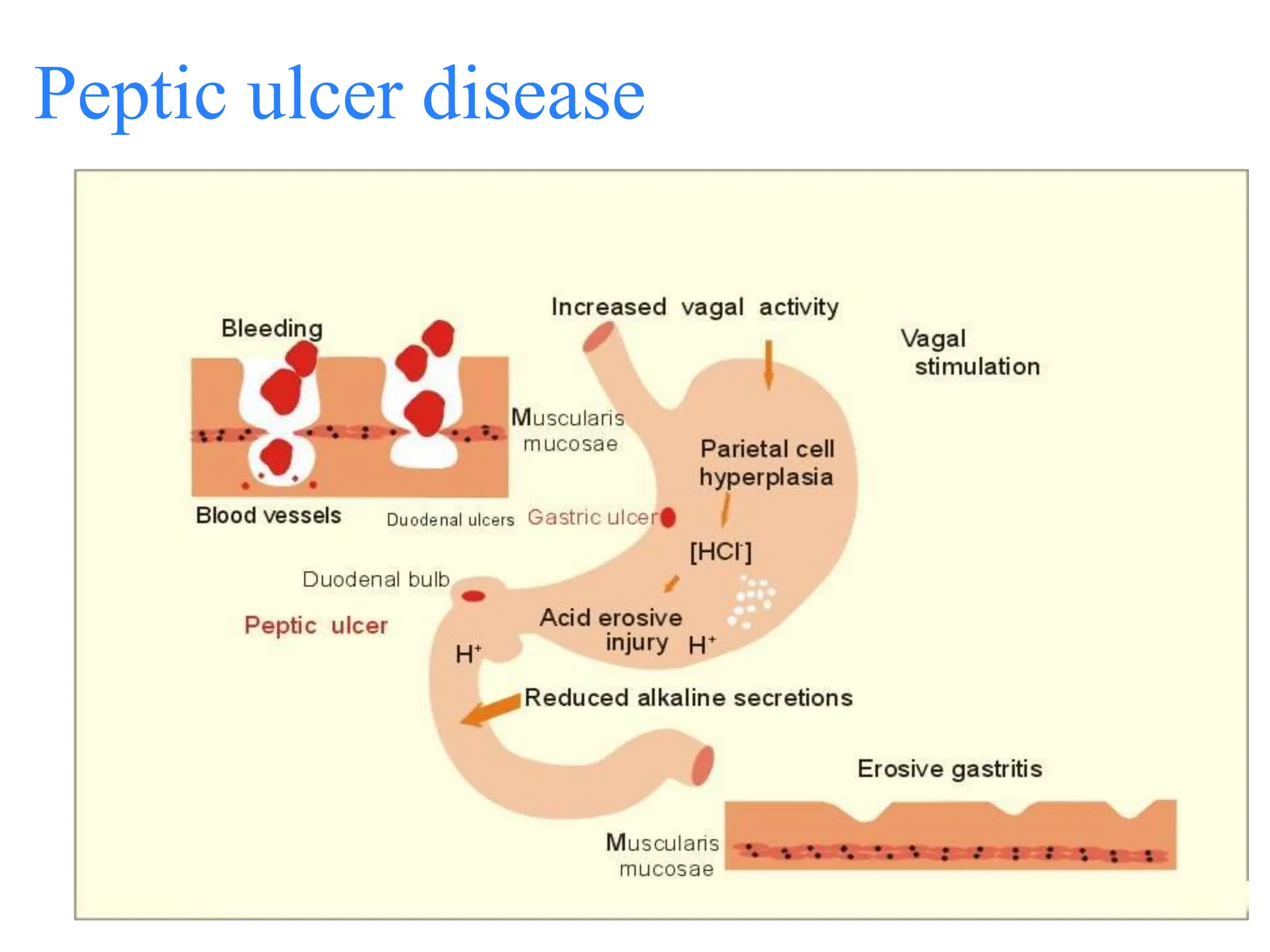
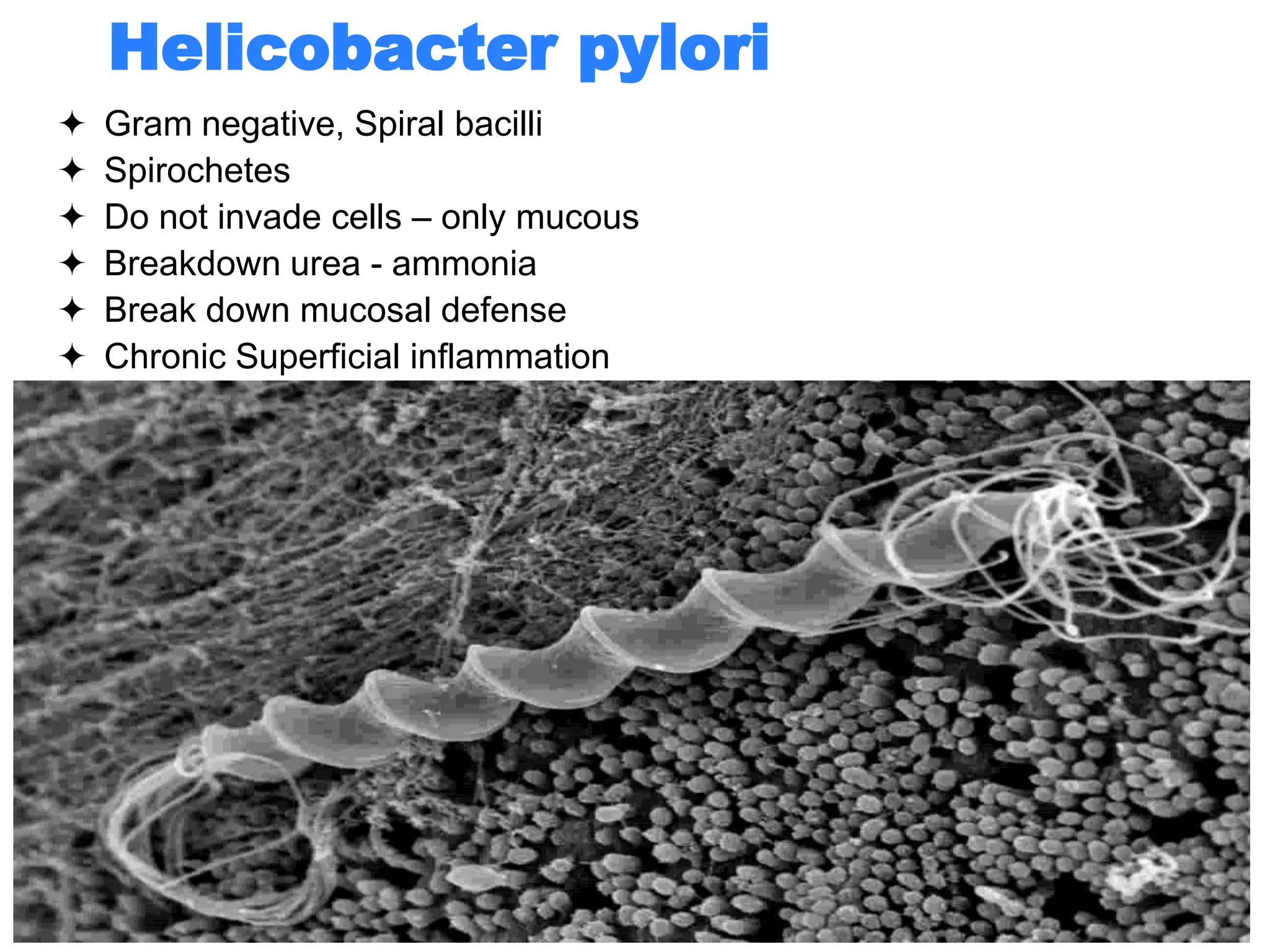
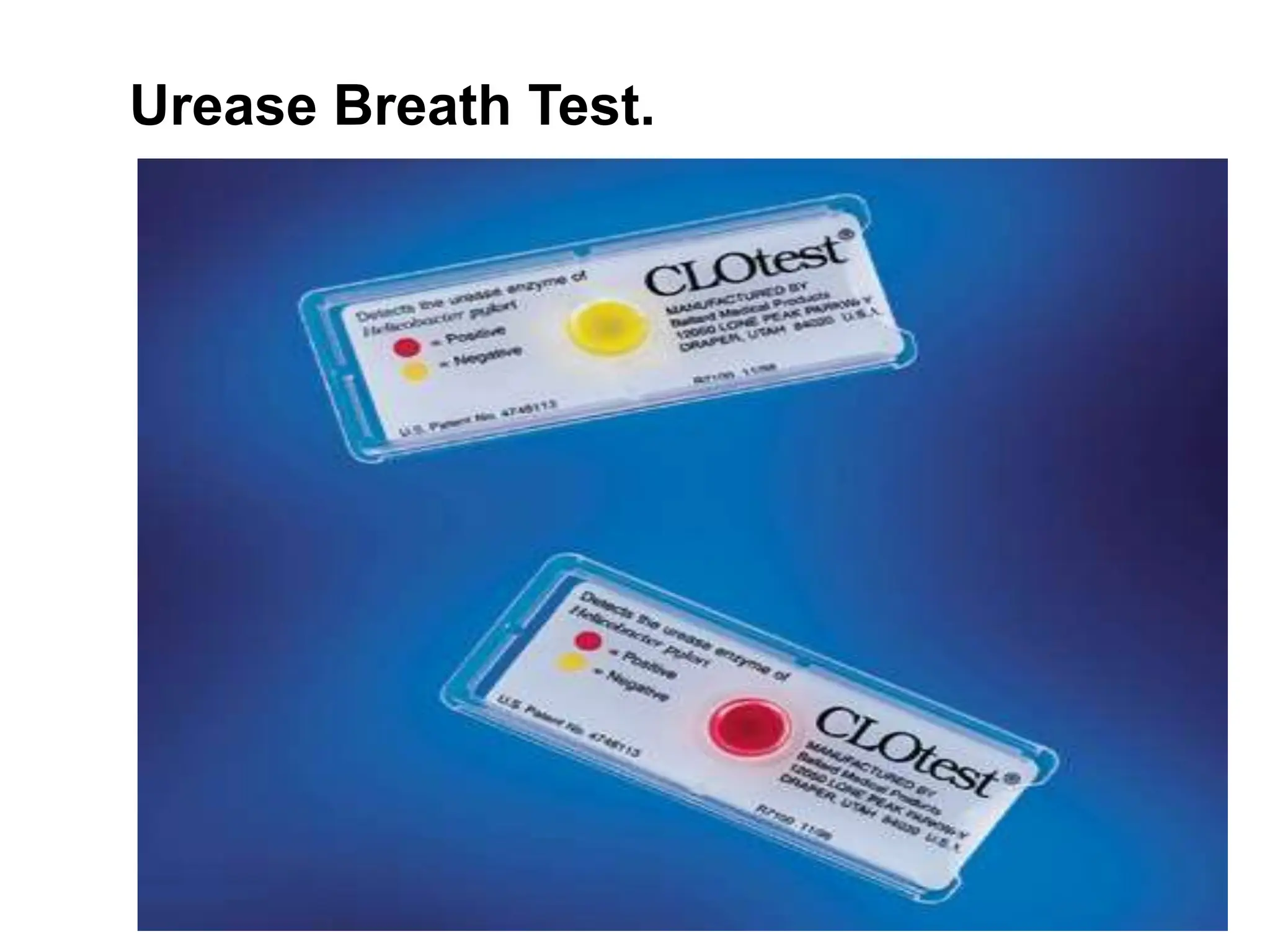
The document discusses peptic ulcer disease (PUD), defining terms like peptic and gastric ulcers, and outlining etiological factors, including Helicobacter pylori infection, excess acid production, and stress. It details clinical presentation, complications, and diagnostic methods, such as endoscopy and biopsy. Treatment options include non-pharmacological measures, triple therapy, and precautions for dental care to reduce the risk of ulcer complications.