3. Definition of peptic ulcer.
Location and symptoms.
Types.
Etiology.
Pathophysiology and pathogenesis
Signs & symptoms
Complications ,diagnostic studies and treatment.
Precautions.
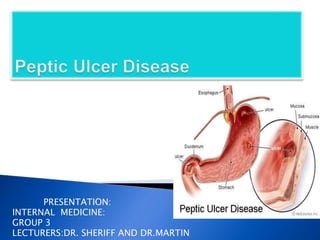
4. • Peptic ulcer disease (PUD) refers to ulceration of the
mucosa anywhere in the GI tract exposed to acid and
pepsin.
• Ulcers : breaks in the mucosal surface >5 mm, with depth
to the sub-mucosa.
• They can range in size from a few millimeters to a few
centimeters
• The 2 most common forms/locations of PUD are
– Duodenal ulcer
– Gastric ulcer
Site
• Lower esophagus
• Stomach
• Duodenum
5. Under normal conditions, a physiologic balance
exists between gastric acid secretion and
gastroduodenal mucosal defense. Mucosal injury
and, thus, peptic ulcer occur when the balance
between the aggressive factors and the defensive
mechanisms is disrupted. Aggressive factors,
such as NSAIDs, H pylori infection, alcohol, bile
salts, acid, and pepsin, can alter the mucosal
defense by allowing back diffusion of hydrogen
ions and subsequent epithelial cell injury.
10. Helicobacter pylori (HP) is a spiral shaped,
gram negative, flagellated bacteria first
associated with PUD in the early 1980’s
Found in most people with duodenal and
gastric ulcers
◦ About 95% of those with duodenal ulcers
◦ About 80% of those with gastric ulcers
HP is primarily spread through the fecal to oral
route
Oral – oral routes
Through contaminated food and water
People are most often infected during
childhood
11. Mechanisms by which HP causes mucosal injury
are not entirely clear but occurs through a
combination of the following mechanisms:
◦ HP catalyzes urea ammonia is produced ammonia
erodes the mucous barrier and causes epithelial damage
◦ HP produces cytotoxins
◦ HP produces mucolytic enzymes
PATHOGENESIS
12. In long-term NSAID users, there is a 10% - 20%
prevalence of gastric ulcers and a 2% - 5% prevalence
of duodenal ulcers
Mechanisms for NSAID-induced ulceration
◦ NSAIDs are weak acids and are non-ionized at gastric
pH
Diffuse freely across the mucous barrier into gastric
epithelial cells H+ ions are liberated and cause cellular
damage
• Aspirin is the most ulcerno-genic of all NSAIDs.
– Even with low dose aspirin (81-162mg/day), ulcers
occur in 0.6% - 1.2% of patients per year
13. • NSAIDs inhibit cyclooxygenase activity and
therefore decrease prostaglandin
production which results in a:
Reduction in gastric and mucosal blood
flow
Decrease in mucous and bicarbonate
secretion
Decrease in cellular repair and replication
14. • ZES is characterized by gastric acid
hypersecretion and recurrent peptic ulcers that
result from a gastrin-producing tumor
–More than 50% of gastrinomas are malignant
• ZES is suspected for patients with multiple
ulcers and recurrent or refractory PUD often
accompanied by esophagitis or ulcer
complications
• Only accounts for 0.1% to 1% of those with
duodenal ulcer
15. • Cigarette smoking
– Impairs ulcer healing and increases the risk of
recurrence
• Psychological stress
– Stress may induce behavioral risks such as
smoking and the use of NSAIDs or may alter the
inflammatory response or resistance to HP
infection
• Dietary factors
– Certain foods (e.g. coffee, tea, carbonated
beverages, beer, milk, spices) may cause
dyspepsia but do not increase the risk of
developing PUD
16. Signs &Symptoms
Abdominal discomfort usually occurs in epigastric area
(upper middle part of the abdomen) radiating to the back
described as:
dull gnawing ache comes and goes for several days
pain may increase when the stomach is empty at night or
half to three hours after meal.
Pain is relieved by eating & antacid medication.
Weight change
Fatigue
Bloating
Chest pain
Burping
Nausea and Anorexia (common with gastric ulcer)
Vomiting (relieves episodes of severe pain due to evacuation
of gastric acid content).
Heart burn
17. Emergency symptoms:
If you have any of these symptoms call your
doctor right away:
Sharp sudden persistent abdominal pain.
Bloody or black stools.
Bloody vomit or vomit that looks like coffee
grounds.
Dysphagia
They could be signs of a serious problem such as:
Perforation when the ulcer burrows through
the stomach or duodenal wall.
18.
19. Less common than duodenal ulcers
◦ Especially in chronic NSAID use
Most commonly located in the lesser curvature of the antrum of the
stomach
More common in people greater than 60 years old
Characterized by
• A normal to low secretion of gastric acid
• Back diffusion of acid is greater (chronic )
• Critical pathologic process is amount of acid able to penetrate mucosal barrier
• H pylori is present in 50% to 70%
• Drugs --- Aspirin, corticosteroids, N SAIDs, reserpine, Chronic alcohol abuse,
chronic gastritis
20. Most common form of PUD
◦ It is 3 times more common than gastric ulcers
Usually located in the duodenal bulb of the small
intestine
Most commonly occurs in people between the
ages of 30 and 50
Associated with ↑HCl acid secretion
H.pylori associated in 9 0- 9 5 % of cases
Diseases with ↑risk of duodenal ulcers
COPD, cirrhosis of liver, chronic pancreatitis,
hyperparathyroidism, chronic renal failure
21. 3 major complications
Hemorrhage - 15% of patients with active PUD
Perforation - 7% of patients with active PUD
Gastric outlet obstruction
Initially treated conservatively
May require surgery at any time during
course of therapy
22.
23.
24. The second most common ulcer – related
complications is perforation( occur in 6-7% of
PUD patients)
Dus tend to penetrate posteriorly in to the
pancrease, leading to pancreatitis, whereas
Gus tend to penetrate in to the left hepatic
lobe.
25. Gastric outlet obstruction is the least
common ulcer-related
complications,occuring in 1-2% of patients
26. Endoscopy procedure
◦ Determines degree of ulcer healing after treatment
◦ Tissue specimens can be obtained to identify H. pylori and to rule
out gastric cancer
Tests for H.pylori
◦ Noninvasive tests
Serum or whole blood antibody tests
Immunoglobin G (I g G)
Urea breath test
C 14 breath test
Fecal antigen test
◦ Invasive tests
Biopsy of stomach
Rapid urease test
27. The urea breath and fecal antigen tests may be
falsely negative in patients who have recently
taken
◦ Antibiotics (up to 4 weeks)
◦ Bismuth compounds (up to 4 weeks)
◦ Antisecretory agents (up to 2 weeks)
28. Barium contrast studies
◦ Widely used
X- ray studies
◦ Ineffective in differentiating a peptic ulcer from a
malignant tumor
29.
30. Medical regimen consists of
◦ Adequate rest
◦ Dietary modification
◦ Drug therapy
◦ Elimination of risk factors
◦ Long-term follow-up care
32. Histamine receptor blocks (H2 R blockers)-
famotidine,cimetidine
Used to manage peptic ulcer disease
Block action of histamine on H2 receptors
↓ HCl acid secretion
↓ conversion of pepsinogen to pepsin
↑ ulcer healing
Proton pump inhibitors – pantoprazole,
rabeprazole
◦ Block ATPase enzyme that is important for secretion
of HCl acid
Antibiotic therapy
◦ Eradicate H. pylori infection
◦ No single agents have been effective in eliminating H.
pylori
33. Antacids – calcium carbonate, MgOH
◦ Used as adjunct therapy for peptic ulcer disease
◦ ↑ gastric pH by neutralizing acid
Anticholinergic drugs- Dicyclomine
◦ Occasionally ordered for treatment
◦ ↓ cholinergic stimulation of HCl acid
• Bismuth preparations
• Agents
– Bismuth subsalicylate
– Bismuth exhibits antimicrobial activity against
bacterial and viral gastrointestinal pathogens
34. Standard triple therapy regimen contains
◦ Amoxicillin 1000mg twice day + Clarithromycin 500mg
twice a day + a PPI dosed once to twice a day
◦ Given for 10 to 14 days
14 day regimens are generally preferred as 14 day
regimens significantly increases the eradication rate
Bismuth-based quadruple-therapy contains
◦ Tetracycline 500mg 4 times day +Metronidazole 250-
500mg 2/3 times a day + Bismuth subsalicylate 525mg 4
times a day + a PPI once or twice a day OR H2-receptor
antagonist twice a day
35. • When symptoms, ulcers, or both persist beyond 8
to 12 weeks despite conventional treatment as
previously described or when several courses of H.
pylori eradication therapy fail
• Patient should undergo an upper endoscopy to
assess the situation
• Treatment depends on cause and may include
additional H. pylori eradication attempts, higher PPI
dosages, or surgery
36. Dietary modifications may be necessary so that
foods and beverages irritating to patient can be
avoided or eliminated
Protein considered best neutralizing food
◦ Stimulates gastric secretions
Carbohydrates and fats are least stimulating to
HCl acid
secretion
◦ Do not neutralize well
37. < 20% of patients with ulcers need
surgical intervention
Indications for surgical interventions
Intractability
History of hemorrhage, ↑ risk of bleeding
Prepyloric or pyloric ulcers
Multiple ulcer sites
Drug-induced ulcers
Possible existence of a malignant ulcer
Obstruction