Downloaded 112 times




![PID Curriculum
7
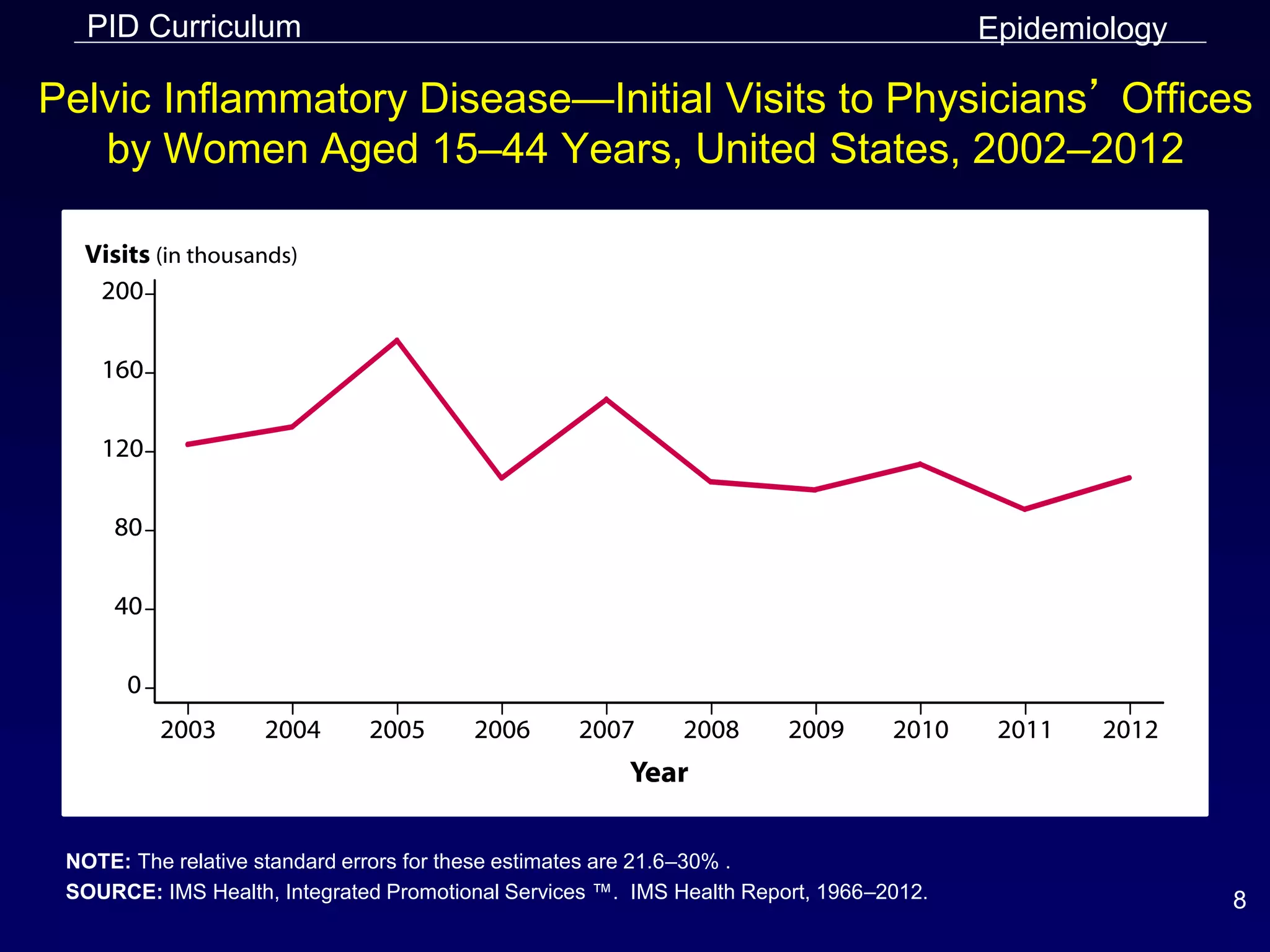
Pelvic Inflammatory Disease—Hospitalizations of Women
Aged 15–44 Years, United States, 2001–2010
NOTE: The relative standard errors for acute and unspecified pelvic inflammatory disease (PID) cases ranges from
8%-18%. The relative standard error for chronic PID cases ranges from 12%–28%. Data only available through
2010.
SOURCE: 2010 National Hospital Discharge Survey [Internet]. Atlanta: Centers for Disease Control and Prevention.
Available from: http://www.cdc.gov/nchs/nhds.htm.
Epidemiology](https://image.slidesharecdn.com/pid-slides-2014-151005103837-lva1-app6892/75/Pelvic-Inflammatory-Disease-Case-study-patterns-and-association-7-2048.jpg)




























This document provides information on Pelvic Inflammatory Disease (PID) in a curriculum format. It covers the epidemiology, pathogenesis, clinical manifestations, diagnosis, patient management, and prevention of PID. The learning objectives are to describe various aspects of PID including the epidemiology in the US, clinical criteria for diagnosis, CDC treatment guidelines, and prevention strategies. The curriculum contains 7 lessons that cover these topics in detail with examples and illustrations to enhance understanding of PID.











































































































