Downloaded 60 times

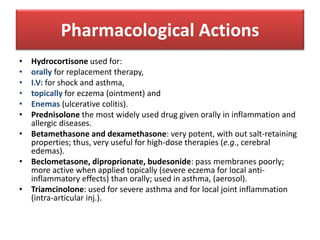
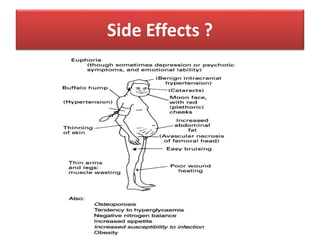

This document discusses types, routes of administration, pharmacological actions, and guidelines for weaning oral corticosteroids. It describes corticosteroid types including replacement therapy drugs like hydrocortisone and mineralocorticoid like fludrocortisone. It also discusses anti-inflammatory corticosteroids that can be short, intermediate, or long acting when administered systemically or locally. The document provides details on specific drugs and their uses, as well as a multi-step process for slowly weaning off oral corticosteroids to avoid withdrawal symptoms.























































































