Downloaded 219 times
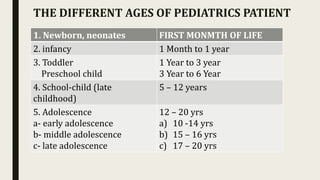
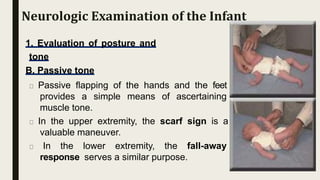
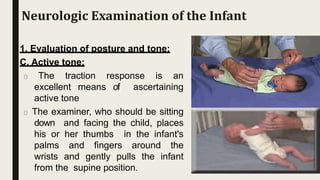
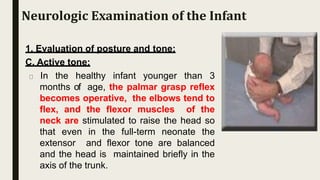
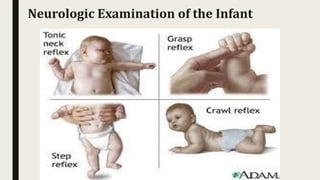
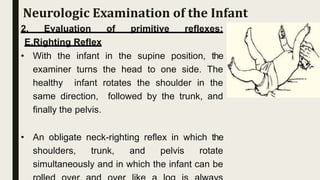

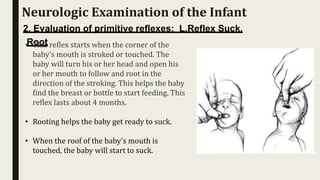


This document provides information on examining the nervous system in pediatric patients of different ages. It discusses the approaches and techniques used, which vary depending on the age of the child. For infants, the examination focuses on evaluating posture, tone, and primitive reflexes. It is important to observe developmental abilities and note any abnormalities. The neurologic and developmental examinations should proceed together in infants. The document outlines the assessment of various reflexes and tones in an infant neurological examination.






















































































