The document provides registry data from Monroe Carell Jr. Children's Hospital at Vanderbilt for 2015, including:
- Total trauma admissions were 1117, with 19 deaths and 7 organ donors.
- The non-surgical admission rate was 3%, overtriage rate was 47%, and undertriage rate was 11%.
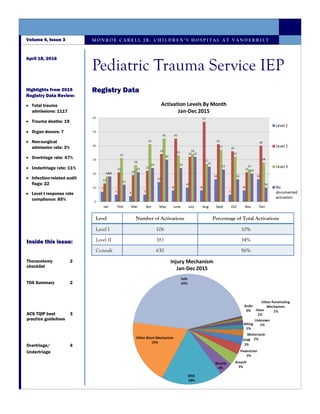
- Level I trauma activations made up 10% of total activations, with Level II at 34% and consult at 56%.
Learn about the principles behind the surgical checklist and the evidence for adopting the checklist and how one NHS Board has applied the checklist to their surgical theatres and how another has expanded the checklist principle to other areas.
Learn about the principles behind the surgical checklist and the evidence for adopting the checklist and how one NHS Board has applied the checklist to their surgical theatres and how another has expanded the checklist principle to other areas.
WHO has undertaken a number of global and regional initiatives to address surgical safety. The Global Initiative for Emergency and Essential Surgical Care and the Guidelines for Essential Trauma Care focussed on access and quality. The Second Global Patient Safety Challenge: Safe Surgery Saves Lives addresses the safety of surgical care.
Major incidents - what can we learn from them?scanFOAM
A talk by Sabina Fattah at the 2017 meeting of the Scandinavian Society of Anaestesiology and Intensive Care Medicine.
All available content from SSAI2017: https://scanfoam.org/ssai2017/
Delivered in collaboration between scanFOAM, SSAI & SFAI.
Improving Surgical Safety and Patient OutcomesC Daniel Smith
Keynote talk delivered at New Jersey Hospital Association Seminary on Improving Surgical Safety & Patient Outcomes held on September 25, 2013 at their Conference Center in Princeton New Jersey. Over physicians, administrators, nurses and perioperative services providers in attendance.
1. Safety is everybody’s business. According the Hippocratic oath from 5th century : “ Never do harm to anyone” Safer Surgery can be defined as a reduction in avoidable harm to a surgical patient
2. It is a part of medical specialty that uses operative manual and instrumental technique on a patient to investigate or treat a pathological condition. Surgical team: 1. Surgeon 2. Surgeon’s assistance 3. Anesthetist 4. Scrub nurse 5. Scouting nurse 6. Surgical technologist
3. Time or duration when patient admitted and discharge after completion of surgery. So, surgical safety has broadly included in different phases: 1. Preoperative(Diagnosis, investigation) 2. Per operative 3. Postoperative(Up to discharge)
4. 1. Adverse events: An incident which result in harm to the patient. 2. Near Miss: An incident which could resulted in unwanted harm but did not. 3. No-harm events: An incident that occur and reach to the patient but result in no injury.
5. An article in the Gurdian newspaper UK in March 2013 claimed that “five worst medical” nightmares a Pt faces, three related to surgery: 1. Wrong site surgery 2. Wrong patient surgery 3. Retained instruments and swabs The rate of harm in surgical patient is unknown but probably occur in about 10% surgical patient, though much of this harm will be minor.
6. 1. Patients themselves. 2. Healthcare professional 3. System failure. 4. Medical complexity
7. Patients Themselves 1. A variety of presentation. 2. Differing co-morbidities 3. Differing response to treatment 4. Patients are reluctant to speak up. 5. Refuse to co-operate 6. Hide and seek
8. Healthcare professional 1. Inadequate Pt assessment(delay or error in Diagnosis) 2. Failure to use or interpret appropriate test 3. Error in performance of an operation and test. 4. Inadequate monitoring or follow-up. 5. Deficient training or experience 6. Fatigue, overwork or time pressure. 7. Personal or psychological factor i.e. drug abuse or depression. 8. Lack of recognition of the danger of medical errors.
9. System failure 1. Poor communication between healthcare provider. 2. Inadequate staffing level 3. Overreliance on investigation 4. Lack of coordination at handover 5. Drug similarities. 6. Equipment failure due to lack of skilled operators. 7. Inadequate system to report and review patient safety incident.
10. Medical complexity 1. Advance and new technologies(laparoscopic, robotic surgery) 2. Potent drug and their side effects and interaction. 3. Working environment- Surgical ICU, HDU and Operation theatre
11. Surgery is one of the most complex health intervention to deliver. More than 100 million people worldwide require surgical treatment every year for different reason. Great Professor of Surgery Sir Alfred Cuschieri and other describes surgical errors in different categories that committed by the surgeons during care of the Patients.
12. 1. Diagnosis and management erro
Presentation at the Health Consumers Council Patient Experience Week Events, by Dr Carmel Crock and Ms Anita Deakin.
The Emergency Medicine Events Register is an "adverse event and near-miss reporting system that is peer-led, online, anonymous and confidential. It is a means of supporting improvement in safety and quality in emergency medicine by understanding of contributing factors and how the risk of harm to patients can be minimised or prevented."
See http://www.emer.org.au/
The World Health Organisation is a global tool to ensure safety in surgery. The principles and procedures are described for how to implement it in your organisation.
This presentation was done by RUTAYISIRE François Xavier and ISHIMWE Diane, medical students at University of RWANDA School of Medicine and pharmacy, department of medicine and surgery. They did it while they were in Year 4 (Doctorate2), under supervision of Dr Ntakiyiruta Georges,Mmed,FCSECSA. It tell us about what a surgical safety checklist is, and why is it important in surgical field.
WHO has undertaken a number of global and regional initiatives to address surgical safety. The Global Initiative for Emergency and Essential Surgical Care and the Guidelines for Essential Trauma Care focussed on access and quality. The Second Global Patient Safety Challenge: Safe Surgery Saves Lives addresses the safety of surgical care.
Major incidents - what can we learn from them?scanFOAM
A talk by Sabina Fattah at the 2017 meeting of the Scandinavian Society of Anaestesiology and Intensive Care Medicine.
All available content from SSAI2017: https://scanfoam.org/ssai2017/
Delivered in collaboration between scanFOAM, SSAI & SFAI.
Improving Surgical Safety and Patient OutcomesC Daniel Smith
Keynote talk delivered at New Jersey Hospital Association Seminary on Improving Surgical Safety & Patient Outcomes held on September 25, 2013 at their Conference Center in Princeton New Jersey. Over physicians, administrators, nurses and perioperative services providers in attendance.
1. Safety is everybody’s business. According the Hippocratic oath from 5th century : “ Never do harm to anyone” Safer Surgery can be defined as a reduction in avoidable harm to a surgical patient
2. It is a part of medical specialty that uses operative manual and instrumental technique on a patient to investigate or treat a pathological condition. Surgical team: 1. Surgeon 2. Surgeon’s assistance 3. Anesthetist 4. Scrub nurse 5. Scouting nurse 6. Surgical technologist
3. Time or duration when patient admitted and discharge after completion of surgery. So, surgical safety has broadly included in different phases: 1. Preoperative(Diagnosis, investigation) 2. Per operative 3. Postoperative(Up to discharge)
4. 1. Adverse events: An incident which result in harm to the patient. 2. Near Miss: An incident which could resulted in unwanted harm but did not. 3. No-harm events: An incident that occur and reach to the patient but result in no injury.
5. An article in the Gurdian newspaper UK in March 2013 claimed that “five worst medical” nightmares a Pt faces, three related to surgery: 1. Wrong site surgery 2. Wrong patient surgery 3. Retained instruments and swabs The rate of harm in surgical patient is unknown but probably occur in about 10% surgical patient, though much of this harm will be minor.
6. 1. Patients themselves. 2. Healthcare professional 3. System failure. 4. Medical complexity
7. Patients Themselves 1. A variety of presentation. 2. Differing co-morbidities 3. Differing response to treatment 4. Patients are reluctant to speak up. 5. Refuse to co-operate 6. Hide and seek
8. Healthcare professional 1. Inadequate Pt assessment(delay or error in Diagnosis) 2. Failure to use or interpret appropriate test 3. Error in performance of an operation and test. 4. Inadequate monitoring or follow-up. 5. Deficient training or experience 6. Fatigue, overwork or time pressure. 7. Personal or psychological factor i.e. drug abuse or depression. 8. Lack of recognition of the danger of medical errors.
9. System failure 1. Poor communication between healthcare provider. 2. Inadequate staffing level 3. Overreliance on investigation 4. Lack of coordination at handover 5. Drug similarities. 6. Equipment failure due to lack of skilled operators. 7. Inadequate system to report and review patient safety incident.
10. Medical complexity 1. Advance and new technologies(laparoscopic, robotic surgery) 2. Potent drug and their side effects and interaction. 3. Working environment- Surgical ICU, HDU and Operation theatre
11. Surgery is one of the most complex health intervention to deliver. More than 100 million people worldwide require surgical treatment every year for different reason. Great Professor of Surgery Sir Alfred Cuschieri and other describes surgical errors in different categories that committed by the surgeons during care of the Patients.
12. 1. Diagnosis and management erro
Presentation at the Health Consumers Council Patient Experience Week Events, by Dr Carmel Crock and Ms Anita Deakin.
The Emergency Medicine Events Register is an "adverse event and near-miss reporting system that is peer-led, online, anonymous and confidential. It is a means of supporting improvement in safety and quality in emergency medicine by understanding of contributing factors and how the risk of harm to patients can be minimised or prevented."
See http://www.emer.org.au/
The World Health Organisation is a global tool to ensure safety in surgery. The principles and procedures are described for how to implement it in your organisation.
This presentation was done by RUTAYISIRE François Xavier and ISHIMWE Diane, medical students at University of RWANDA School of Medicine and pharmacy, department of medicine and surgery. They did it while they were in Year 4 (Doctorate2), under supervision of Dr Ntakiyiruta Georges,Mmed,FCSECSA. It tell us about what a surgical safety checklist is, and why is it important in surgical field.
Vans Triple Crown of Surfing Announced by William Michael Gallant; TallahasseeWilliam Michael Gallant
William Michael Gallant of Tallahassee, Florida is a surfer who has traveled around the world for adventure and for the best possible places to surf. This presentation is about the Vans Triple Crown event within the surf world.
Samples of Competitive Examination Questions: Part XXXXIXAli I. Al-Mosawi
كتاب (نماذج أسئلة الإمتحان التنافسي/ إعداد علي إبراهيم الموسوي)
الجزء التاسع والأربعون:
ماجستير لغة عربية قسم اللغة العربية كلية العلوم الإسلامية جامعة بغداد ... ماجستير إجتماع قسم علم الإجتماع كلية الآداب جامعة بغداد ... ماجستير كيمياء قسم الكيمياء كلية العلوم جامعة القادسية ... ماجستير كيمياء قسم الكيمياء كلية العلوم جامعة تكريت ... دكتوراه كيمياء قسم الكيمياء كلية العلوم جامعة تكريت.
“Por una comunidad donante: para compartir el corazón y algo mas…””
Universidad Nacional de Misiones
Facultad de Humanidades y Ciencias Sociales –
Secretaria de Extension: CEPRODITx (Res. Nº 170/09 )
Directora: Mag. Marta Espínola - Docente – investigadora - Extensionista Fac. de Hum. Y Cs. Ss. Directora CEPRODITx
La disuasión se logra en base a una concatenación de medidas técnicas, comportamiento y conceptos CPTED, que tienen su origen en el pensamiento racional del ser humano (raciocinio, creencias, vivencias y actitud).
El delincuente es una persona racional, que toma decisiones racionales. Su pensamiento racional le indica que por encima del botín, no quiere ser visto, ni detenido. Las medidas de protección físicas le generan dificultades técnicas, de tiempo y de esfuerzo físico, lo que le disuade del intento, ante el más que probable fracaso de su intento. El delincuente profesional quiere trabajar cada día.
40%-80% of auto accident claimants have overlooked diagnoses. The most commonly overlooked are thoracic outlet syndrome, cervical disc damage mistakenly called sprain or whiplash, post-concussion syndrome, slipping rib syndrome, Tietze syndrome and Tempro-mandibular joint syndrome. This article tells readers the clinical sign and symptoms of each and the correct medical tests to use, which are employed by doctors at Johns Hopkins Hospital. It also described an on-line questionnaire at www.DiagnoseThePains.com which gives diagnoses with a 96% correlation with diagnoses of Johns Hopkins Hospital doctors.
Missed Diagnoses association in Rear end collisions Nelson Hendler
There are a number of overlooked diagnoses which occur after a rear-end accident. This paper shows an attorney how to convert a misdiagnosed 'soft tissue injury case" into damaged cervical disc,TMJ, thoracic outlet syndrome,and post concussion syndrome using a diagnostic paradigm to get diagnoses with a 96% correlation with diagnoses of Johns Hopkins Hospital doctors. This improves patient care and increases recovery.
Operation “Blue Star” is the only event in the history of Independent India where the state went into war with its own people. Even after about 40 years it is not clear if it was culmination of states anger over people of the region, a political game of power or start of dictatorial chapter in the democratic setup.
The people of Punjab felt alienated from main stream due to denial of their just demands during a long democratic struggle since independence. As it happen all over the word, it led to militant struggle with great loss of lives of military, police and civilian personnel. Killing of Indira Gandhi and massacre of innocent Sikhs in Delhi and other India cities was also associated with this movement.
The Roman Empire A Historical Colossus.pdfkaushalkr1407
The Roman Empire, a vast and enduring power, stands as one of history's most remarkable civilizations, leaving an indelible imprint on the world. It emerged from the Roman Republic, transitioning into an imperial powerhouse under the leadership of Augustus Caesar in 27 BCE. This transformation marked the beginning of an era defined by unprecedented territorial expansion, architectural marvels, and profound cultural influence.
The empire's roots lie in the city of Rome, founded, according to legend, by Romulus in 753 BCE. Over centuries, Rome evolved from a small settlement to a formidable republic, characterized by a complex political system with elected officials and checks on power. However, internal strife, class conflicts, and military ambitions paved the way for the end of the Republic. Julius Caesar’s dictatorship and subsequent assassination in 44 BCE created a power vacuum, leading to a civil war. Octavian, later Augustus, emerged victorious, heralding the Roman Empire’s birth.
Under Augustus, the empire experienced the Pax Romana, a 200-year period of relative peace and stability. Augustus reformed the military, established efficient administrative systems, and initiated grand construction projects. The empire's borders expanded, encompassing territories from Britain to Egypt and from Spain to the Euphrates. Roman legions, renowned for their discipline and engineering prowess, secured and maintained these vast territories, building roads, fortifications, and cities that facilitated control and integration.
The Roman Empire’s society was hierarchical, with a rigid class system. At the top were the patricians, wealthy elites who held significant political power. Below them were the plebeians, free citizens with limited political influence, and the vast numbers of slaves who formed the backbone of the economy. The family unit was central, governed by the paterfamilias, the male head who held absolute authority.
Culturally, the Romans were eclectic, absorbing and adapting elements from the civilizations they encountered, particularly the Greeks. Roman art, literature, and philosophy reflected this synthesis, creating a rich cultural tapestry. Latin, the Roman language, became the lingua franca of the Western world, influencing numerous modern languages.
Roman architecture and engineering achievements were monumental. They perfected the arch, vault, and dome, constructing enduring structures like the Colosseum, Pantheon, and aqueducts. These engineering marvels not only showcased Roman ingenuity but also served practical purposes, from public entertainment to water supply.
Ethnobotany and Ethnopharmacology:
Ethnobotany in herbal drug evaluation,
Impact of Ethnobotany in traditional medicine,
New development in herbals,
Bio-prospecting tools for drug discovery,
Role of Ethnopharmacology in drug evaluation,
Reverse Pharmacology.
How to Make a Field invisible in Odoo 17Celine George
It is possible to hide or invisible some fields in odoo. Commonly using “invisible” attribute in the field definition to invisible the fields. This slide will show how to make a field invisible in odoo 17.
Unit 8 - Information and Communication Technology (Paper I).pdfThiyagu K
This slides describes the basic concepts of ICT, basics of Email, Emerging Technology and Digital Initiatives in Education. This presentations aligns with the UGC Paper I syllabus.
How to Split Bills in the Odoo 17 POS ModuleCeline George
Bills have a main role in point of sale procedure. It will help to track sales, handling payments and giving receipts to customers. Bill splitting also has an important role in POS. For example, If some friends come together for dinner and if they want to divide the bill then it is possible by POS bill splitting. This slide will show how to split bills in odoo 17 POS.
Students, digital devices and success - Andreas Schleicher - 27 May 2024..pptxEduSkills OECD
Andreas Schleicher presents at the OECD webinar ‘Digital devices in schools: detrimental distraction or secret to success?’ on 27 May 2024. The presentation was based on findings from PISA 2022 results and the webinar helped launch the PISA in Focus ‘Managing screen time: How to protect and equip students against distraction’ https://www.oecd-ilibrary.org/education/managing-screen-time_7c225af4-en and the OECD Education Policy Perspective ‘Students, digital devices and success’ can be found here - https://oe.cd/il/5yV
This is a presentation by Dada Robert in a Your Skill Boost masterclass organised by the Excellence Foundation for South Sudan (EFSS) on Saturday, the 25th and Sunday, the 26th of May 2024.
He discussed the concept of quality improvement, emphasizing its applicability to various aspects of life, including personal, project, and program improvements. He defined quality as doing the right thing at the right time in the right way to achieve the best possible results and discussed the concept of the "gap" between what we know and what we do, and how this gap represents the areas we need to improve. He explained the scientific approach to quality improvement, which involves systematic performance analysis, testing and learning, and implementing change ideas. He also highlighted the importance of client focus and a team approach to quality improvement.
We all have good and bad thoughts from time to time and situation to situation. We are bombarded daily with spiraling thoughts(both negative and positive) creating all-consuming feel , making us difficult to manage with associated suffering. Good thoughts are like our Mob Signal (Positive thought) amidst noise(negative thought) in the atmosphere. Negative thoughts like noise outweigh positive thoughts. These thoughts often create unwanted confusion, trouble, stress and frustration in our mind as well as chaos in our physical world. Negative thoughts are also known as “distorted thinking”.
Digital Tools and AI for Teaching Learning and Research
Pediatric Trauma IEP Newsletter April 2016
1. Registry Data
M O N R O E C A R E L L J R . C H I L D R E N ’ S H O S P I T A L A T V A N D E R B I L T
April 18, 2016
Volume 4, Issue 3
Pediatric Trauma Service IEP
Highlights from 2015
Registry Data Review:
Total trauma
admissions: 1117
Trauma deaths: 19
Organ donors: 7
Non-surgical
admission rate: 3%
Overtriage rate: 47%
Undertriage rate: 11%
Infection-related audit
flags: 22
Level I response rate
compliance: 85%
Inside this issue:
Thoracotomy
checklist
2
TDS Summary 2
ACS TQIP best
practice guidelines
3
Overtriage/
Undertriage
4
Level Number of Activations Percentage of Total Activations
Level I 106 10%
Level II 381 34%
Consult 630 56%
2. Family conversations:
According to Federal regulations, the
family of each potential donor is to be
informed of their loved one’s
opportunity to donate. Per your
hospital’s policy, TDS is the designated
party responsible for presenting the
opportunity of donation.
During the organ donation process, the
hospital and OPO will develop a plan
for the opportunity of donation to be
presented to the family, or discuss the
registered donor options, at the most
appropriate time.
Triggers:
It is the responsibility of the patient’s
nurse or designee to contact TDS
within one hour of a patient first
meeting one of the following clinical
indicators:
GCS ≤5 due to condition/illness
Beginning discussion of end of life
and/or withdrawal
Organ donation is no longer an option
when a patient is extubated. Always
notify TDS if the patient’s medical
status declines or if the plan of care
changes.
Pathways:
There are two pathways to donation
that can take place at the end of life.
Donation after Brain Death
TDS will input orders as the
Attending Physician, StarPanel
chart will change to Donor, Last
Name
Donation after Circulatory Death
Patient will remain under the
care of ICU Attending and work
in conjunction with TDS to input
orders. Name will not change.
Thoracotomy Checklist
Tennessee Donor Services
Page 2
Pediatric Trauma Service IEP
PED Thoracotomy Checklist
Pre-arrival actions Immediate actions
Thoracotomy tray out on mayo stand Patient’s left arm positioned above their head
10 blade and handle out on mayo stand Left chest painted with betadine
Procedural lights ON and positioned at proceduralist’s pref-
erence
Procedure lights focused on left chest
Betadine at bedside Move mayo stand within arm’s reach of proceduralist
Notify OR of procedure possibility and request assistance Open thoracotomy tray and place within arm’s reach of
Yankuer suction catheter and suction canister devoted to
procedure
ETT placed by PED team
OR blue towels NGT/OGT placed by RN3
Standby items (open upon trauma leaders request)
Activation of MTP Level I infuser
10ml syringes 16fr foley catheter
Central line kit Sutures
The PED will be adding the following checklist to the thoracotomy tray cabinet to assist in expediting the procedure.
3. Background:
> 60% of injuries involve the musculoskeletal system.
> 50% of hospitalized trauma patients have at least one musculoskeletal injury that could be life threatening, limb threatening,
or result in significant functional impairment.
Orthopaedic injuries are often associated with significant health care costs, decreased productivity in the workplace, and, in
some cases, long-term disability.
Open fractures:
Patients with open fractures receive intravenous antibiotics within 60 minutes of presentation to your ED.
All patients with open fractures are evaluated for the potential need for tetanus vaccination.
Patients with open fractures are taken to the operating room for surgical irrigation and debridement within 24 hours of
presentation to your ED.
Mangled extremity:
All patients who present to the emergency department with a mangled extremity undergo prompt orthopaedic evaluation (as
defined by institutional protocol).
All patients with a mangled extremity have timely (as defined by institutional protocol) operative management.
Compartment syndrome:
All patients diagnosed with compartment syndrome who require an amputation of the involved extremity are identified and
reviewed by the trauma PIPS or equivalent committee within the hospital.
Pelvic trauma/ associated hemorrhage:
Patients with hemorrhage from pelvic fractures are evaluated promptly by orthopaedics (as defined by institutional protocols)
A team with angiographic capabilities is consulted and promptly (as defined by institutional protocols) evaluates all patients
with pelvic fractures, evidence of contrast extravasation on cross-sectional imaging, and either hemorrhage or hemodynamic
stability.
Supracondylar humerus fractures
All patients with radiographic evidence of a supracondylar humerus fracture are promptly (as defined by institutional protocol)
evaluated by an orthopaedic surgeon
All patients with supracondylar fractures who do not receive timely management (for example, surgical repair within 18 hours
for Gartland Type III fractures) are identified and reviewed by the trauma PIPS or equivalent committee within the hospital.
Any patient with evidence of global forearm dysfunction or ischemia following supracondylar humerus fracture is identified
and reviewed in the trauma PIPS or equivalent committee within the hospital.
Rehabilitation of the multisystem trauma patient:
All delays in discharge of multisystem trauma patients due to inadequate or unavailable rehabilitation services are identified
and reviewed by the trauma PIPS or equivalent committee within the hospital.
Current Orthopaedic metrics being collected on the ACS application:
Time to IV antibiotics for open fractures should be less than 1 hour from presentation to your ED (and # of pts).
Time to operative I+D (not ER or ICU) for open tibia fractures should be less than 24 hours from presentation to your ED.
The percent of femoral shaft fractures (shaft only) treated with an IMN, plate and screws, or external fixation within 24 hours
of presentation to your ED.
ACS TQIP Orthopaedic Best Practice Guidelines
Page 3
Volume 4, Issue 3
4. Definitions:
Undertriage is a level II/III activation or “no activation” with an injury severity score (ISS) 16-75 call divided by the total
patients with “limited” or “no activation”. Other factors to consider in the definition of a major trauma patient may include
those requiring blood transfusion as part of their initial resuscitation or requiring intubation, intensive care unit admission,
emergent surgery or interventional catheter-based control of hemorrhage, or intracranial pressure monitoring.
Overtriage is the level I trauma activation with an ISS 0-15 cell divided by the total patients with level I activations.
ACS criteria pertaining to overtriage and under triage:
Rigorous multidisciplinary performance improvement is essential to evaluate overtriage and undertriage rates to attain the
optimal goal of less than 5 percent undertriage (CD 3–3). Undertriage cases should be reviewed in depth.
Rates of undertriage and overtriage must be monitored and reviewed quarterly (CD 16–7).
Injury severity score:
The Injury Severity Score (ISS) is an anatomical scoring system that provides an overall score for patients with multiple injuries.
Each injury is assigned an Abbreviated Injury Scale (AIS) score and is allocated to one of six body regions (Head, Face, Chest,
Abdomen, Extremities (including Pelvis), External). Only the highest AIS score in each body region is used. The 3 most severely
injured body regions have their score squared and added together to produce the ISS score.
An example of the ISS calculation is shown below:
Review of undertriage/overtriage cases:
Our PM&I committee reviews undertriage/overtriage rates monthly and these rates are also shared with our FlightCom/
LifeFlight staff.
Each case is reviewed with the FlightCom manager to look for areas of opportunity.
In the majority of cases, the identified opportunity is attributed to one of the following:
Pre-hospital crew’s failure to report specific injuries or abnormal vital signs.
MCJCHV level I or level II criteria not followed leading to either overtriage or undertriage.
Criteria misinterpreted or taken to the extreme (i.e.– dog bite to face considered penetrating injury to the head).
Proposed solution:
Education sessions with FlightCom provided by both the Trauma Program Manager and CRPC/Outreach team.
TPM component will focus on the criteria itself and identifying proper activation levels based on criteria.
Monroe Carell Jr. Children’s Hospital at Vanderbilt
Overtriage and Undertriage
Region Injury Description AIS Square Top Three
Head & Neck Cerebral contusion 3 9
Face No injury 0
Chest Flail chest 4 16
Abdomen
Minor contusion of liver
Complex rupture of spleen
2
5
25
Extremity Fractured femur 3
External No injury 0
50Injury Severity Score