
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (19)
Similar to Feb 2016 iep
Similar to Feb 2016 iep (20)
More from skrentz
Recently uploaded
Recently uploaded (20)
Feb 2016 iep
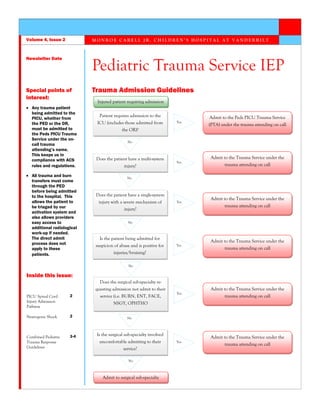
- 1. Trauma Admission Guidelines M O N R O E C A R E L L J R . C H I L D R E N ’ S H O S P I T A L A T V A N D E R B I L T Newsletter Date Volume 4, Issue 2 Pediatric Trauma Service IEP Special points of interest: Any trauma patient being admitted to the PICU, whether from the PED or the OR, must be admitted to the Peds PICU Trauma Service under the on- call trauma attending’s name. This keeps us in compliance with ACS rules and regulations. All trauma and burn transfers must come through the PED before being admitted to the hospital. This allows the patient to be triaged by our activation system and also allows providers easy access to additional radiological work-up if needed. The direct admit process does not apply to these patients. Inside this issue: PICU Spinal Cord Injury Admission Pathway 2 Neurogenic Shock 2 Combined Pediatric Trauma Response Guidelines 3-4 Injured patient requiring admission Patient requires admission to the ICU (includes those admitted from the OR)? Does the patient have a multi-system injury? No Yes Admit to the Peds PICU Trauma Service (PTA) under the trauma attending on call No Yes Admit to the Trauma Service under the trauma attending on call Is the patient being admitted for suspicion of abuse and is positive for injuries/bruising? No Yes Admit to the Trauma Service under the trauma attending on call Does the surgical sub-specialty re- questing admission not admit to their service (i.e. BURN, ENT, FACE, NSGY, OPHTHO Yes Admit to the Trauma Service under the trauma attending on call No Is the surgical sub-specialty involved uncomfortable admitting to their service? No Does the patient have a single-system injury with a severe mechanism of injury? Admit to surgical sub-specialty No Yes Admit to the Trauma Service under the trauma attending on call Yes Admit to the Trauma Service under the trauma attending on call
- 2. hypothermia. Decreased systemic vascular resistance results in relative hypovolemia due to the increased venous capacity. Treatment: The hypotension that results from loss of autonomic tone can precipitate further secondary ischemic injury to the spinal cord. To combat this, it should initially be treated with crystalloid or colloid fluids until the team is able to rule out the possibility of hemorrhage. Hypotension due to neurogenic shock often requires the addition of vasopressors since it is often refractory to Neurogenic shock is classified as a form of distributive shock but should be used as a diagnosis of exclusion in the early phases of trauma resuscitation after hemorrhagic shock is ruled out. (1) Symptoms: Patients classically exhibit hypotension and relative bradycardia. This bradycardia is often exacerbated by suctioning, turning, and hypoxia. Initially skin is often warm and flushed due to profound vasodilation. Heat loss may occur making the patient prone to fluid resuscitation. If bradycardia is present, patients may respond to Atropine, Glycopyrrolate, or vasoactive infusions with chronotropic, vasoconstrictor, and inotropic properties such as Dopamine or Norepinephrine. Complications: Complete injuries or higher grade injuries often lead to more severe neurogenic shock. In addition, the presence of neurogenic shock has been shown to lead to delays in operative management, which may potentially worsen outcomes as well. PICU Spinal Cord Injury Admission Pathway Neurogenic Shock Page 2 Pediatric Trauma Service IEP Admission Service/ Attending Peds PICU Trauma Service Trauma attending on call Spine NSGY ORTHO Labs CBC QAM (HCT>21%) BMP QAM Radiological Studies MRI total spine Lateral c-spine (post halo placement) Monitoring Q1H: VS, Neuro, Sensation checks MAP goals x 5 days <3yr; 60 3-12yr: 70 13-16yr: 75 >16yr: 80 Strict I/O Normocapnia Arterial BP monitoring Accuchecks Q2H (glucose between 80- 150) Vasopressors Dopamine Epinephrine Norepinephrine Neosynephrine Medications Fentanyl Versed Remifentanil Fluids D5 1/2 NS with 20 mEq KCL D5 NS with 20 mEq KCL Diet NPO (24hr) TF (advance to goal) Diet as tolerated Activity Bedrest on KenAir Mattress Strict log rolling only, HOB flat Turn/reposition Q2H DVT Prophylaxis SCD in place (on 2hr/ off 2hr) TED hose in place Bladder Indwelling catherter x 24-48hr In and out cath Q6H Consults PT/OT Speech (swallow) Rehab Services 1. Mack, E. (2013). Neurogenic Shock. The Open Pediatric Medicine Journal, 16-18.
- 3. With the recent update in trauma center criteria, ACS identified the need define specific response times based on the needs of the patient and the trauma team. Below are the specific criteria that speaks to these additions: Neurotrauma care must be continuously available for all TBI and spinal cord injury patients and must be present and respond within 30 minutes based on institutional-specific criteria (CD 8–2). Ortho must be available in the trauma resuscitation area within 30 minutes after consultation has been requested by the surgical trauma team leader for multiply injured patients (CD 9-7) based on institution-specific criteria. Response parameters for consultants addressing time-critical injuries (for example, epidural hematoma, open fractures, and hemodynami- cally unstable pelvic fractures) must be determined and monitored (CD 5–16). The Trauma Operational Process Performance Improvement Committee (TOPPIC) worked together in collaboration with their various services to define our institutional-specific criteria at the end of 2015. The below guidelines are the result of this group’s work. They will be monitored by our trauma registry and reported out as necessary. Combined Pediatric Trauma Response Guidelines Pediatric Trauma Service 1. The Pediatric Trauma Service (attending or fellow) will be available in the resuscitation area within 15 minutes of patient arrival for Level I trauma activations. The attending or fellow serves as the team leader and directs the overall trauma resuscitation. All orders will come from the team leader during the trauma resuscitation. It is expected that the attending or fellow surgeon will be in the emergency department on patient arrival, with adequate notification from the field. The maximum acceptable response time is 15 minutes for the highest-level activation, tracked from patient arrival. A resident in PGY 3/4 or a PEM attending who is part of the trauma team may be approved to begin initial resuscitation while awaiting the arrival of the attending surgeon but cannot independently fulfill the responsibilities of, or substitute for, the attending surgeon or fellow. The presence of such a resident or attending emergency physician may allow the attending or fellow surgeon to take call from outside the hospital. 2. The Pediatric Trauma Service (PGY ≥1) will be available in the resuscitation area within 30 minutes of patient arrival for Level II trauma activations. The PEM attending, PEM fellow, or Trauma senior resident serves as the team leader and directs the overall trauma resuscitation. All orders will come from the team leader during the trauma resuscitation. It is expected that the surgery resident or NP/PA will be in the emergency department on patient arrival, with adequate notification from the field. The maximum acceptable response time is 30 minutes for the midlevel-level activation, tracked from patient arrival. 3. The Pediatric Trauma Service (PGY ≥1) will be available in the resuscitation area within 1 hour after consultation has been requested by the PEM team leader for Level III activations and Trauma consults. Pediatric Spine Service 1. The Pediatric Spine Service (PGY ≥2 or NP) will be available in the trauma resuscitation area within 30 minutes after consultation has been requested by the surgical trauma team leader for the following situations: Increasing neurologic deficit Unstable cervical spine CONTINUED ON FOLLOWING PAGE... Page 3 Volume 4, Issue 2
- 4. Pediatric Neurosurgery Service 1. The Pediatric Neurosurgical Service (PGY 3/4, or NP) will be available in the trauma resuscitation area within 30 minutes after consultation has been requested by the surgical trauma team leader for the following situations: Evidence of increased intracranial pressure as evidenced by a GCS≤8 with: Unilateral blown pupil OR Head CT with signs of impending or active herniation 2. The Pediatric Neurosurgical Service (PGY 3/4, or NP) will be available in the trauma resuscitation area within 30 minutes after consultation has been requested by the surgical trauma team leader for the following situations: Acute epidural hematoma (EDH) The optimal time for addressing EDH cases in need of surgical intervention is within four hours of injury. The decision to operate on an acute EDH is based on the patient’s GCS score, pupillary exam, comorbidities, CT findings, age, and, in delayed decisions, the patient’s ICP. Neurological deterioration over time is also an important factor influencing the decision to operate. Consultation should take place once a head CT has been obtained or uploaded from an outside facility. Acute subdural hematoma (SDH) The optimal time for addressing SDH cases in need of surgical intervention is within four hours of injury. The decision to operate on an acute SDH is based on the patient’s GCS score, pupillary exam, comorbidities, CT findings, age, and, in delayed decisions, the patient’s ICP. Neurological deterioration over time is also an important factor influencing the decision to operate. Consultation should take place once a head CT has been obtained or uploaded from an outside facility. Pediatric Orthopaedic Service 1. The Pediatric Orthopaedic Service (PGY2/3) will be available in the trauma resuscitation area within 30 minutes after consultation has been requested by the surgical trauma team leader for the following situations: Acute limb compartment syndrome Pulseless extremity 2. The Pediatric Orthopaedic Service (PGY2/3) will be available in the trauma resuscitation area within 1 hour after consultation has been requested by the surgical trauma team leader for the following situations: Open fractures All open fractures irrespective of type require urgent irrigation and debridement (I&D). The optimal time for addressing these cases is within eight hours from injury. If the patient cannot be taken to the OR within eight hours of injury due to problems with clearance by trauma surgery or neurosurgery, a preliminary I&D will be performed at the bedside to decrease the amount of gross contamination. Once medical clearance is obtained, the patient will then be taken to the Operating Room for I&D of the open fracture. The Orthopaedic resident on-call is responsible for performing the bedside I&D of the open fracture as well as splinting the fracture for stabilization. Antibiotics will be initiated by the resident per protocol. Hemodynamic instability related to long bone or pelvic fractures Consultation should take place once fluid resuscitation has been initiated by the Pediatric Trauma Service. Pediatric Surgical Specialties (ALL) 1. All surgical specialties will be available in the trauma resuscitation area within 30 minutes after consultation has been requested by the surgical team leader for patients whose condition deteriorates. Monroe Carell Jr. Children’s Hospital at Vanderbilt