







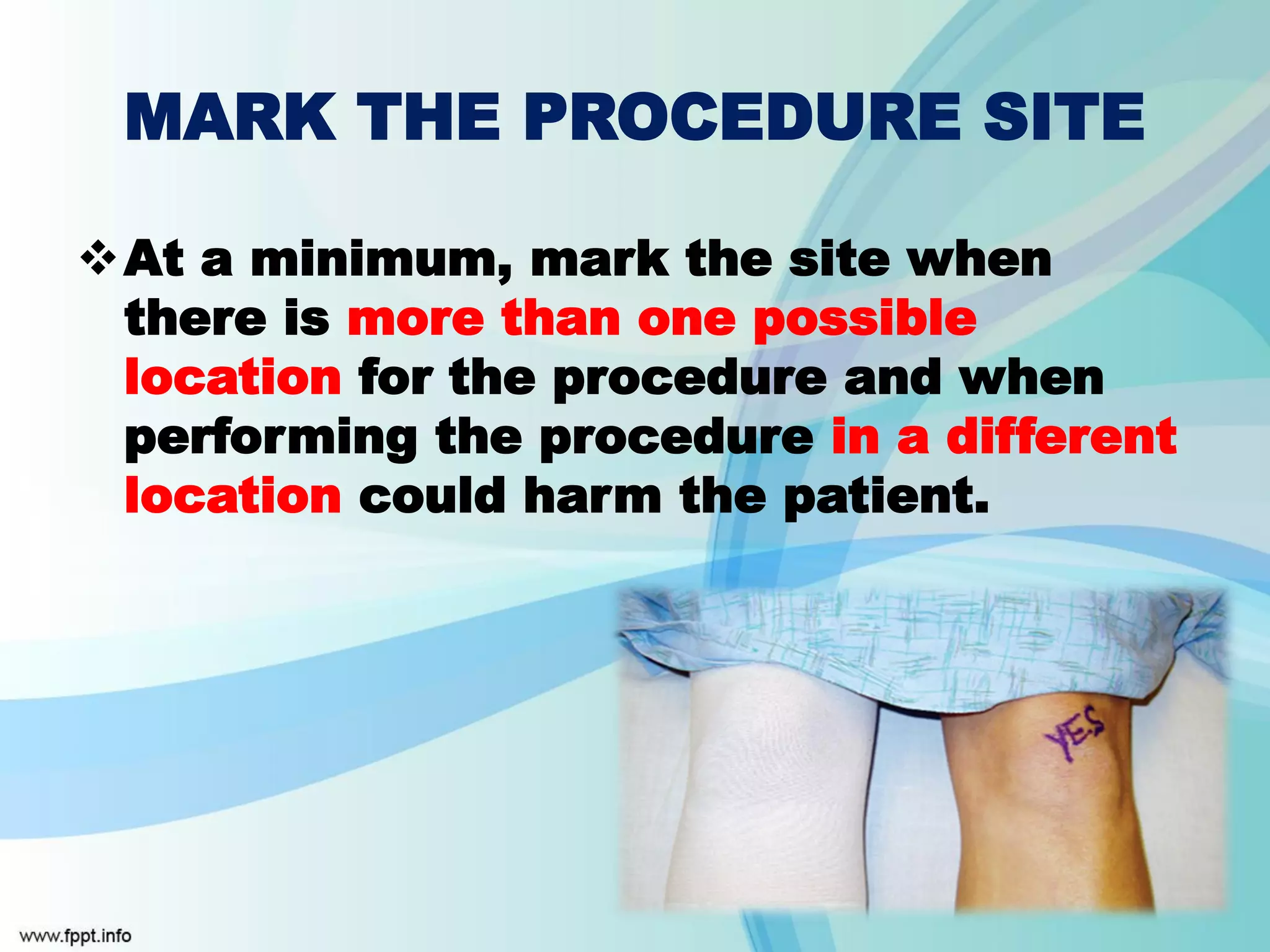





The Universal Protocol is a set of procedures implemented in 2004 to prevent wrong site, wrong procedure, and wrong patient surgery. It includes three key elements: pre-procedure verification, marking the intended site, and conducting a time-out immediately before starting the procedure. The goal is to use data on adverse events collected by JCI to prevent similar errors in other healthcare organizations.





































































































