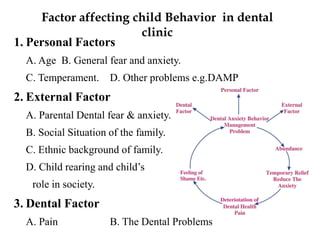


This document discusses psychological growth and development in children from infancy to adolescence. It covers the key periods of development and important behaviors and milestones at each stage. For example, it notes that infancy from birth to 1 year is a critical period for personality development and trust building. It also discusses common behaviors seen in children during dental visits, such as crying, anxiety, resistance and timidity. The document provides several classifications of child behaviors and factors that can influence their behavior, such as their age, dental experiences and parental influences. It emphasizes the importance of effective communication and behavior management techniques in caring for children, such as modeling, positive reinforcement and distraction.























































































