Download to read offline
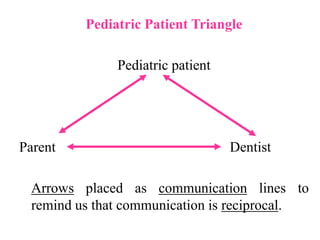









The document discusses the significance of psychological management in pediatric dentistry, emphasizing the importance of understanding child behavior to create a positive dental experience. It outlines developmental milestones for children, behavior patterns in the dental office, and factors influencing their behavior, such as parental attitudes and past experiences. The content highlights the unique relationship between the dentist, child, and parent, illustrating the need for effective communication and management strategies tailored to each child's needs.







![[Pedo] restorative dentistry](https://cdn.slidesharecdn.com/ss_thumbnails/pedorestorativedentistry-210903140140-thumbnail.jpg?width=640&height=640&fit=bounds)


































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)












