










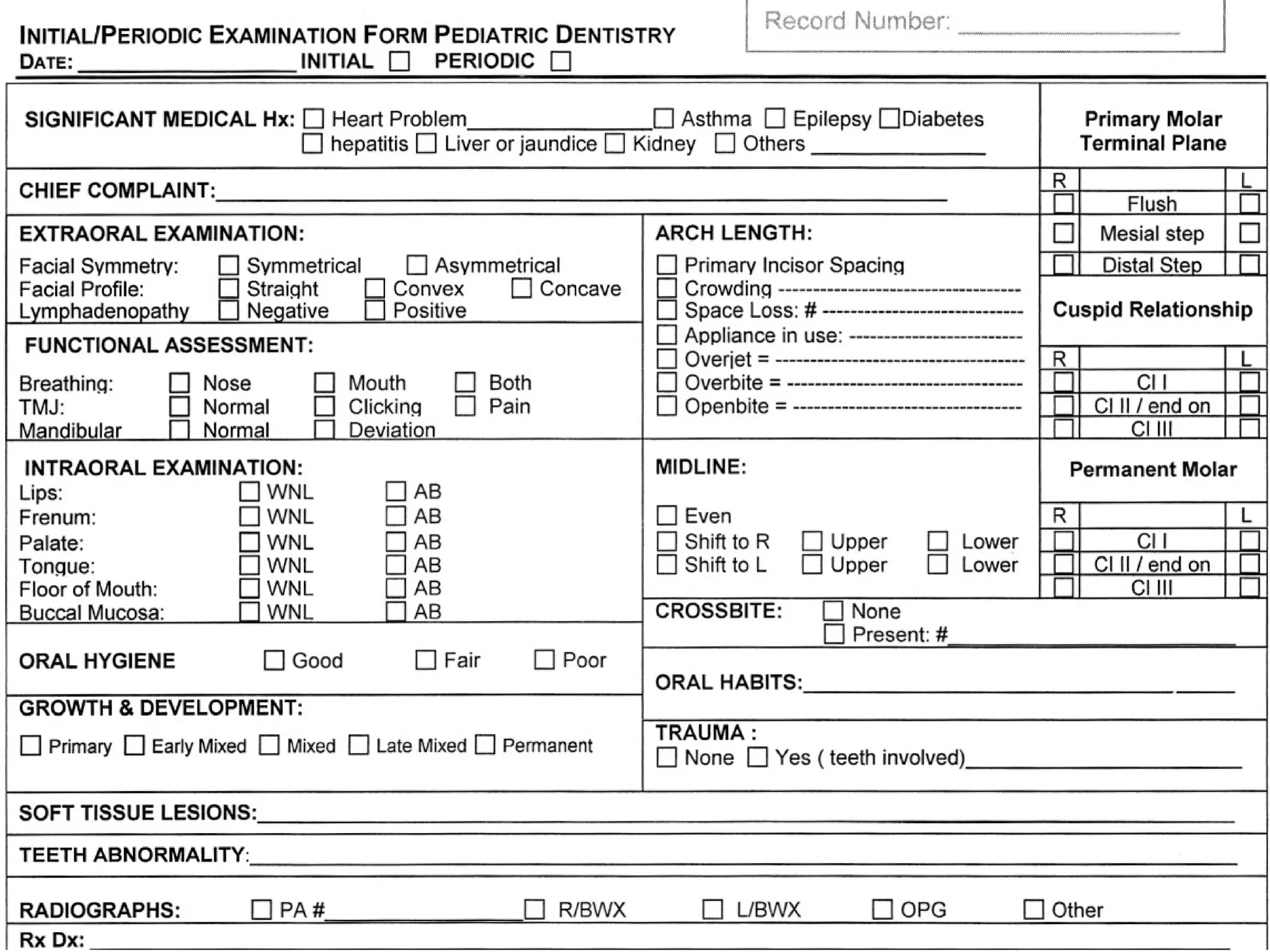






















The document provides guidance on various aspects of conducting examinations and providing treatment for pediatric dental patients. It discusses examining and recording a patient's medical and dental history, performing clinical and radiographic examinations, developing treatment plans, providing preventive care and treating issues like caries. The goal is to properly diagnose any oral health problems, educate parents, prevent future issues, and promote proper development and maintenance of the primary and permanent dentitions.