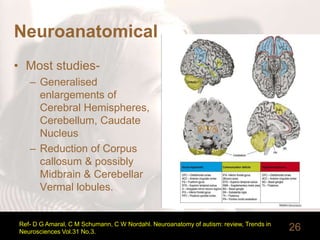
The document discusses pervasive developmental disorders and autism spectrum disorders. It presents a case vignette of a 5-year-old boy named Donald exhibiting symptoms of autism such as lack of social interaction and affection. It then covers the history of autism including theorists who studied and named different conditions. It discusses diagnostic classifications, prevalence, potential etiologies including genetic and neurological factors, and features of autistic disorder.