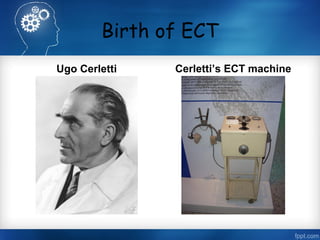
This document discusses the history and procedure of electroconvulsive therapy (ECT). It begins by defining ECT as the application of electric current to the head to induce a seizure for improving abnormal mental states. It then outlines the early history of inducing seizures for psychiatric treatment from the 16th century through various chemical methods. It describes the development of ECT in the 1930s-1940s by Cerletti and Bini who applied electricity directly to humans. The document covers the mechanisms, electrical principles, electrode placements, indications, contraindications, pretreatment, effects and risks of the modern ECT procedure.