Downloaded 60 times

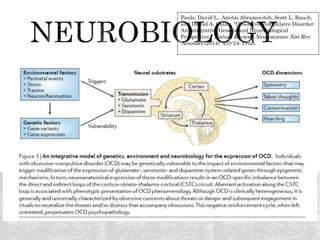
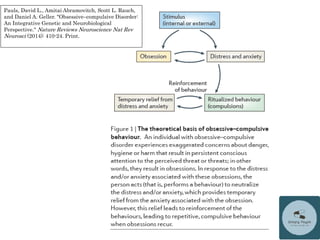
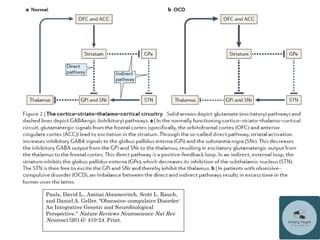



This document is a lecture on obsessive compulsive disorder (OCD) and related disorders given by Dr. Michael Ingram. The lecture introduces OCD, including definitions of obsessions and compulsions. It reviews the epidemiology, diagnosis, neurobiology, and treatment of OCD. It also briefly discusses other OCD spectrum disorders like body dysmorphic disorder, hoarding disorder, trichotillomania, and excoriation disorder. The goal is for attendees to be able to recognize signs and symptoms of OCD and related disorders, understand the neurobiology of impulsivity and compulsivity, and recall treatment options for OCD and related disorders.



































![Etiopathogenesis of obsessive compulsive disorder [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/etiopathogenesisofobsessivecompulsivedisorderautosaved-170329074058-thumbnail.jpg?width=640&height=640&fit=bounds)
















![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)














