Downloaded 529 times
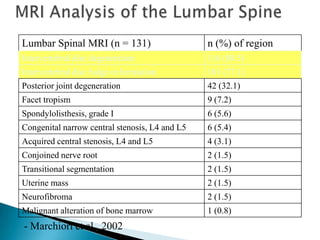
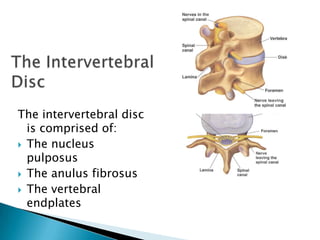
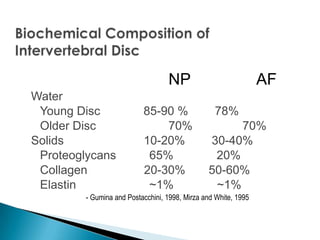


Low back pain is common and disability from back pain is increasing. A lumbar MRI of 131 patients found high rates of intervertebral disc degeneration (88.5%), bulge or herniation (77.1%), and posterior joint degeneration (32.1%). The intervertebral disc consists of the nucleus pulposus and anulus fibrosus, which are derived from the notochord and mesenchymal cells during development. Disc degeneration occurs with aging and is associated with decreased cell density, water content, and proteoglycans in the disc. Genetic factors and mechanical loading influence disc degeneration and herniation risk.






















































































