- Abdulaziz is a 27-year-old man who presented with 7 days of lower back pain after lifting a heavy object. On examination, he had tenderness over the paraspinous muscles and limited forward flexion, but no neurological deficits or red flags.
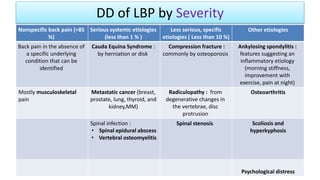
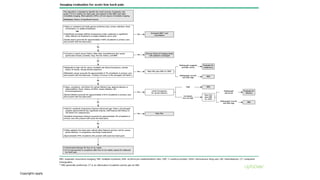
- For patients with nonspecific lower back pain like Abdulaziz without red flags, imaging and other diagnostic tests are not routinely recommended. His history and examination findings are consistent with a diagnosis of back strain.
- The goal of evaluation for lower back pain is to identify red flags indicating serious underlying conditions that require further evaluation or emergent treatment, while Abdulaziz showed no signs of these on history or examination





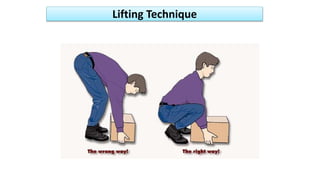
![• Remain active
Advice to stay active recommended and associated with improved
pain and functional status compared to bed rest in patients with acute
low back pain (LBP)
(Strong recommendation, Moderate-quality evidence; level 2 [mid-level] evidence)
• Further education
Benign nature of LBP
Provoking/aggravating factors
If posture → correct, lifting techniques, etc.
54
Patient Education (1)](https://image.slidesharecdn.com/lowbackpainbydr-190308185635/85/Low-back-pain-by-Dr-bagasi-54-320.jpg)
![1. Heat therapy
Associated with short-term pain reduction in patients with acute or
subacute LBP
(level 2 [mid-level] evidence)
No such benefit seen with ice therapy
61
Non-pharmacological (1)](https://image.slidesharecdn.com/lowbackpainbydr-190308185635/85/Low-back-pain-by-Dr-bagasi-61-320.jpg)
![5. Spinal manipulation
o A form of manual therapy that involves the movement of a joint beyond its usual end range
of motion, but not past its anatomic range of motion , high-velocity movement of the joint is
frequently accompanied by an audible cracking or popping sound.
In acute LBP
May reduce pain and disability, but evidenced inconsistent
(level 2 [mid-level] evidence)
In chronic LBP
May slightly improve pain and function at 6 months in patients with chronic LBP.
(level 2 [mid-level] evidence; ACP Strong recommendation, Low-quality evidence)
71
Non-pharmacological (5)](https://image.slidesharecdn.com/lowbackpainbydr-190308185635/85/Low-back-pain-by-Dr-bagasi-71-320.jpg)
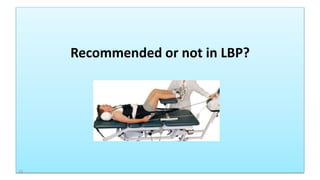
![6. Traction
o Is a form of decompression therapy that relieves pressure on the spine, can be performed
manually or mechanically.
In acute LBP
May provide short-term pain relief in patients with low back pain with or without sciatica.
(level 2 [mid-level] evidence)
In chronic LBP
mechanical traction is not recommended for use in chronic low back pain.
(APS Good-quality evidence)
73
Non-pharmacological (6)](https://image.slidesharecdn.com/lowbackpainbydr-190308185635/85/Low-back-pain-by-Dr-bagasi-73-320.jpg)
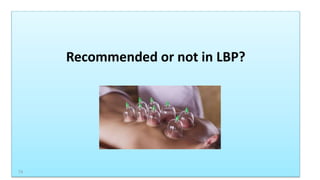
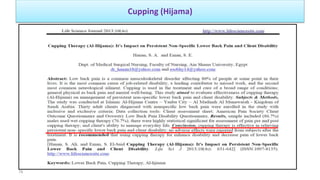
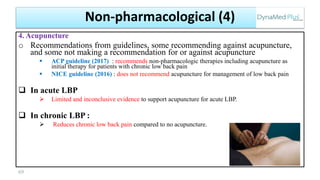
![7. Cupping (Hijama)
o From Sunnah, used for all conditions, especially musculoskeletal pain
Dry pulsatile cupping and minimal cupping may each reduce short term pain in patients with nonspecific
chronic low back pain
(level 2 [mid-level] evidence)
o Based on randomized trial, 110 adults (mean age 49 years) with nonspecific chronic low back pain were
randomized to 1 of 3 interventions for 4 weeks and followed for 12 weeks.
o Result : pulsatile dry cupping and minimal cupping each associated with improved scores on physical component
subscale of Short Form-36 quality-of-life questionnaire compared to control at 4 and 12 weeks.
http://www.dynamed.com/topics/dmp~AN~T906249/Acupuncture-and-related-therapies-for-chronic-low-back-pain#sec-Cupping
76
Non-pharmacological (7)](https://image.slidesharecdn.com/lowbackpainbydr-190308185635/85/Low-back-pain-by-Dr-bagasi-76-320.jpg)
![7. Cupping (Hijama)
Cupping might slightly reduce pain in patients with chronic low back pain
(level 2 [mid-level] evidence)
o Based on systematic review of low-to-moderate quality trials
o 6 trials assessed effect of cupping on patients with low back pain (median treatment duration 3 weeks)
o All trials had ≥ 1 methodologic limitation including unclear randomization, unclear allocation concealment, unclear
blinding of patients and providers, and unclear reporting of dropout rate
o Result :
Cupping associated with slight reduction in pain compared to medication use in analysis of 4 studies with 430
patients
Cupping associated with reduction in pain compared to usual care at 3-month follow-up (in 1 trial with 98 patients
http://www.dynamed.com/topics/dmp~AN~T906249/Acupuncture-and-related-therapies-for-chronic-low-back-pain#sec-Cupping
77
Non-pharmacological (7)](https://image.slidesharecdn.com/lowbackpainbydr-190308185635/85/Low-back-pain-by-Dr-bagasi-77-320.jpg)