OBJECTIVES
• Describe theanatomy of the prostate gland
• Define benign prostate hyperplasia/hypertrophy
• State the causes of BPH
• Describe the pathophysiology of BPH
• Describe the clinical features of BPH
• Discus the management of BPH
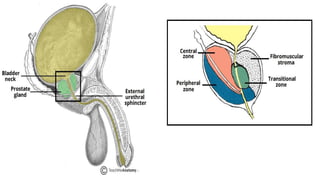
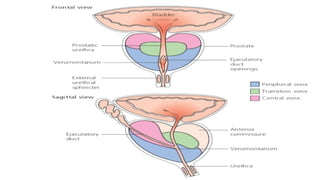
• Central zone– surrounds the ejaculatory ducts, comprising
approximately 25% of normal prostate volume.
• The ducts of the glands from the central zone are obliquely emptying
in the prostatic urethra, thus being rather immune to urine reflux.
• Transitional zone – located centrally and surrounds the urethra,
comprising approximately 5-10% of normal prostate volume.
• The glands of the transitional zone are those that typically undergo
benign hyperplasia (BPH)
6.
• Peripheral zone– makes up the main body of the gland
(approximately 65%) and is located posteriorly.
• The ducts of the glands from the peripheral zone are vertically
emptying in the prostatic urethra; that may explain the tendency of
these glands to permit urine reflux.
• That also explains the high incidence of acute and chronic
inflammation found in these compartments, a fact that may be linked
to the high incidence of prostate carcinoma at the peripheral zone.
7.
• The peripheralzone is mainly the area felt against the rectum on DRE,
which is of irreplaceable value.
FUNCTIONS OF THE PROSTATE
• Releases a milky substance that combines with seminal fluid
and sperm to form semen.
• It secretes proteolytic enzymes into the semen, which act to
break down clotting factors in the ejaculate.
8.
Definition of BPH
•Benign prostate hyperplasia refers to the nonmalignant adenomatous
overgrowth of the periurethral prostate gland.
or
• Benign prostatic hyperplasia (BPH) is the enlargement, or hypertrophy, of
the prostate gland.
• The enlargement causes narrowing of the urethra and results in partial or
complete obstruction.
• It describes a proliferative process of the cellular elements of the prostate, an
enlarged prostate, or the voiding dysfunction resulting from prostatic
enlargement and bladder outlet obstruction.
9.
• It ismuch more common with advancing age, although histological
evidence of hyperplasia may be evident from much earlier ages (<40
yrs old).
• 30- 40 years – 8%
• 50-60 years - 50%
• 80 – 80%
• 100 – 100%
Etiology of BPH
•The cause is not well understood, but evidence suggests hormonal
involvement.
• BPH is influenced by a wide variety of risk factors in addition to direct
hormonal effects of testosterone on prostate tissue.
Risk Factors
1. Genetic Factor
• If a man from one’s immediate family (say for example brother or
father) has been diagnosed with benign prostatic hyperplasia, then
there’s a greater possibility of the man developing the same symptom.
12.
2. Ageing
With ageing,the prostate gland develops a larger size. Hence, the risk of
developing an enlarged prostate becomes apparent. This is significant
for men raging over the age of 50 years. For men who are above 80
years of age, the vast majority will apparently develop an enlarged
prostate gland.
3. The Ethnic Background
Enlarged prostate symptoms might be higher in the black people than in
the white men. Apparently, the reason behind the increased risk might
be because of some genetic differences. Alternatively, the risk might
have to do with some metabolic diseases too which is most common in
the Latinos, Americans, and Africans.
13.
4. People withDiabetes
• A man who has diabetes, has an increased risk of developing an enlarged
prostate gland or BPH. Type 2 diabetes (with high glucose levels) might
increase the progression of benign prostatic hyperplasia. This is due to the
elevated insulin levels.
5. A sedentary Lifestyle
• A sedentary lifestyle or a lack of exercise can also increase the risk of
developing an enlarged prostate. This is due to the fact that exercise helps
in fighting obesity. It also helps in reducing inflammation and the risk of
type 2 diabetes. It also helps insulin resistance and other factors
associated with BPH.
14.
7. People withHeart Diseases -
•The same risks contributing to heart problems also
increase the growth of the prostate. These include
obesity, high blood pressure, and diabetes.
15.
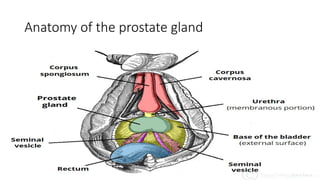
Pathophysiology of benignprostate
hyperplasia
•The prostate consists predominantly of three distinct
zones
•A central zone
•A peripheral zone
•A transition zone, adjacent to the urethra
17.
Pathophysiology cont’d
• BPHdevelops almost exclusively in the transition zone, whereas
prostate cancer usually develops in the peripheral zone.
• The growth and development of the prostate is influenced by the
male hormone testosterone and its more active metabolite
dihydrotestosterone(DHT).
• Testosterone produced in the testes is converted to dihydrotestosterone
(DHT) by the enzyme 5α-reductase 2 in prostate stromal cells.
18.
• DHT hasdirect effects on stromal cells in the prostate, paracrine
effects in adjacent prostatic cells, and endocrine effects in the
bloodstream, which influences both cellular proliferation and
apoptosis (cell death).
• BPH arises as a result of the loss of homeostasis between cellular
proliferation and cell death, resulting in an imbalance favoring cellular
proliferation.
• This results in increased numbers of epithelial and stromal cells in the
periurethral area of the prostate
19.
Pathophysiology cont’d
• BPHarises in the periurethral and transition zones of the prostate.
• Multiple fibroadenomatous nodules develop in the periurethral
region of the prostate, probably originating within the periurethral
glands rather than in the true fibromuscular prostate (surgical
capsule), which is displaced peripherally by progressive growth of the
nodules.
• As the lumen of the prostatic urethra narrows and lengthens, urine
outflow is progressively obstructed.
20.
Pathophysiology cont’d
• Increasedpressure associated with micturition and bladder distention
can progress to hypertrophy of the bladder detrusor, trabeculation,
cellule formation, and diverticula.
• Incomplete bladder emptying causes stasis and predisposes to
calculus formation and infection.
• Prolonged urinary tract obstruction, even if incomplete, can cause
hydronephrosis and compromise renal function.
21.
Symptoms and Signsof BPH
• Lower urinary tract symptoms
These can be divided into;
storage (frequency, nocturia, urgency) and
voiding symptoms (poor stream, straining, hesitancy, prolonged
micturition)
Urinary frequency: Frequent trips to the bathroom to urinate may be an
early sign of a developing BPH.
Urgency: This is the sudden and immediate urge to urinate.
Nocturia: Urinating frequently at night is called nocturia.
• Frequency, urgency, and nocturia are due to incomplete emptying and
rapid refilling of the bladder.
22.
Hesitancy: Difficulty startingor maintaining a urine stream
Intermittency: A urinary stream that is not continuous.
• Decreased size and force of the urinary stream cause hesitancy and
intermittency.
Sensations of incomplete emptying, terminal dribbling, overflow
incontinence, or complete urinary retention may ensue.
23.
Straining to void.This cause congestion of superficial veins
of the prostatic urethra and trigone, which may rupture and
cause hematuria. Straining also may acutely cause vasovagal
syncope and, over the long term, may cause dilation of
hemorrhoidal veins or inguinal hernias.
24.
Urinary retention
Some patientspresent with sudden, complete urinary retention, with
marked abdominal discomfort and bladder distention.
Digital rectal examination
On digital rectal examination, the prostate usually is enlarged and non
tender, has a rubbery consistency, and in many cases has lost the
median furrow.
26.
Diagnosis of BPH
•Digital rectal examination: A DRE often reveals a large, rubbery, and
nontender prostate gland.
• Urinalysis : Color: Yellow, dark brown, dark or bright red (bloody);
appearance may be cloudy. pH 7 or greater (suggests infection);
bacteria, WBCs, RBCs may be present microscopically.
• Urine culture: May reveal Staphylococcus aureus, Proteus, Klebsiella,
Pseudomonas, or Escherichia coli.
27.
• Typically, urinalysisand urine culture are done, and serum prostate-
specific antigen (PSA) levels are measured.
• Prostate-specific antigen level Prostate-specific antigen (PSA):
Glycoprotein contained in the cytoplasm of prostatic epithelial cells,
detected in the blood of adult men. Level is greatly increased in
prostatic cancer but can also be elevated in BPH.
28.
The PSA levelis moderately elevated in 30 to 50% of patients with
BPH, depending on prostate size and degree of obstruction, and is
elevated in 25 to 92% of patients with prostate cancer, depending on the
tumor volume.
In patients without cancer, serum PSA levels > 1.5 ng/mL (1.5 mcg/L)
usually indicate a prostate volume ≥ 30 mL.
If the PSA level is > 4 ng/mL (4 mcg/L), further discussion/shared
decision-making regarding other tests or biopsy is recommended.
29.
• Sometimes uroflowmetryand bladder ultrasonography.
Assesses degree of bladder obstruction. (an objective test of
urine volume and flow rate) with measurement of post void
residual volume by bladder ultrasonography.
• Flow rate < 15 mL/sec suggests obstruction, and post void
residual volume > 100 mL suggests acute retention.
30.
• Other testing
Transrectalbiopsy is usually done with ultrasound guidance (to
minimize risk of infection) and is usually indicated only if there is
suspicion of prostate cancer. Transrectal ultrasonography is an
accurate way to measure prostate volume.
Contrast imaging studies (eg, CT, intravenous urography [IVU]) are
rarely necessary unless the patient has had a urinary tract infection
(UTI) with fever or obstructive symptoms have been severe and
prolonged.
31.
• If anupper tract imaging study is warranted due to pain or elevated
serum creatinine level, ultrasonography may be preferred because it
avoids radiation and IV contrast exposure.
• Alternatively, men whose PSA levels warrant testing can undergo
multiparametric MRI, which is more sensitive (although less specific)
than transrectal biopsy.
• Cystoscopy may help determine the optimal surgical approach and to
rule out other obstructive causes such as strictures.
32.
MANAGEMENT
Medical Management
• Thegoals of medical management of BPH are to improve the quality
of life and treatment depends on the severity of symptoms.
• Catheterization. If a patient is admitted on an emergency basis because
he is unable to void, he is immediately catheterized.
• Cystostomy. An incision into the bladder may be needed to provide
urinary drainage.
33.
• Pharmacologic Management
•Patients with mild to moderate obstructive symptoms, Alpha-
adrenergic blockers (eg. doxazosin, tamsulosin, alfuzosin, terazosin),
which relax the smooth muscle of the bladder neck and prostate may
decrease voiding problems.
• 5alpha reductase inhibitors. Hormonal manipulation with antiandrogen
agents (finasteride [Proscar],dutasteride) decreases the size of the
prostate and prevents the conversion of testosterone to
dihydrotestosterone (DHT).
34.
• A combinationof both classes of drugs is superior to monotherapy.
Possible drug combinations may include; finasteride and doxazosin,
dutasteride and tamsulosin, alpha blockers and antimuscurinic
• For men with concomitant erectile dysfunction, daily tadalafil may
help relieve both conditions.
• One herbal medication effective against BPH is Saw Palmetto.
35.
Surgical Management
• Surgeryis done when patients do not respond to drug therapy or
develop complications such as recurrent urinary tract infection,
urinary calculi, severe bladder dysfunction, or upper tract dilation.
• Transurethral incision of the prostate(TIUP). This is used to widen the
urethra if the prostate gland is small but causes a major blockage.
Small cuts in the bladder neck are made where the urethra joins the
bladder in the prostate. It widens the urethra and reduces the
pressure of the prostate on the urethra, making micturition easier.
36.
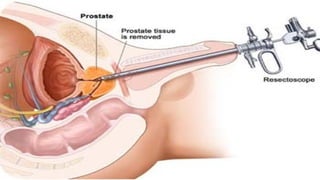
• Transurethral resectionof the prostate (TURP) is the
standard. It uses electric current or laser light to cut and
remove tissue. TURP involves the surgical removal of the
inner portion of the prostate with a resectoscope inserted
through the urethra. The resectoscope provides light,
irrigating fluid and an electrical loop.
38.
• Transurethral needleablation (TUNA). TUNA uses low-level radio
frequencies delivered by thin needles placed in the prostate gland to
produce localized heat that destroys prostate tissue while sparing
other tissues.
• Transurethral microwave heat treatment. It uses microwaves to
destroy prostatic tissue. A urologist inserts a catheter through the
urethra to the prostate. An antenna then sends the micro waves
through the catheter to heat parts of the prostate. A cooling system
protects the urinary tract from damage
39.
• Open prostatectomy.Larger prostates (usually > 75 grams)
traditionally require open surgery via a suprapubic or retropubic
approach.
• Holmium laser enucleation of the prostate (HoLEP) can be done
transurethrally.
40.
Nursing Management
Nursing managementof a patient with BPH includes the following:
• Nursing Assessment
- Nursing assessment focuses on the health history of the patient.
Health history. The health history focuses on the urinary tract,
previous surgical procedures, general health issues, family history of
prostate diseases, and fitness for possible surgery.
Physical assessment. Physical assessment includes digital rectal
examination.
41.
Subjective Data:
• Frequent/ urgent need to urinate, especially at night
• Difficulty urinating or weak urine stream
• Inability to empty the bladder
• Dribbling urine after voiding
• Incontinence
42.
Objective Data:
• ElevatedPSA
• Enlarged prostate on exam or ultrasound
• Inability to pass catheter through urethra
43.
• Nursing Diagnosis
-Based on the assessment data, the appropriate nursing diagnoses for
a patient with BPH are:
Urinary retention related to obstruction in the bladder neck or
urethra.
Acute pain related to bladder distention.
Anxiety related to the surgical procedure.
44.
• Nursing CarePlanning
Relieve acute urinary retention.
Promote comfort.
Prevent complications.
Help patient deal with psychosocial concerns.
Provide information about disease process/prognosis and treatment
needs.
45.
• Nursing Interventions
-Preoperative and postoperative nursing interventions for a patient with
BPH are as follows:
Reduce anxiety. The nurse should familiarize the patient with the
preoperative and postoperative routines and initiate measures to reduce
anxiety.
Relieve discomfort. Bed rest and analgesics are prescribed if a patient
experiences discomfort.
Provide instruction. Before the surgery, the nurse reviews with the patient
the anatomy of the affected structures and their function in relation to the
urinary and reproductive systems.
Maintain fluid balance. Fluid balance should be restored to normal.
Nursing diagnosis PlanningExpected
outcomes
nursing interventions Rationale evaluation
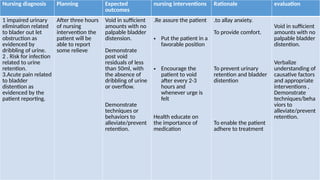
1 impaired urinary
elimination related
to blader out let
obstruction as
evidenced by
dribbling of urine.
2 . Risk for infection
related to urine
retention.
3.Acute pain related
to bladder
distention as
evidenced by the
patient reporting.
After three hours
of nursing
intervention the
patient will be
able to report
some relieve
Void in sufficient
amounts with no
palpable bladder
distension.
Demonstrate
post void
residuals of less
than 50ml, with
the absence of
dribbling of urine
or overflow.
Demonstrate
techniques or
behaviors to
alleviate/prevent
retention.
.Re assure the patient
• Put the patient in a
favorable position
• Encourage the
patient to void
after every 2-3
hours and
whenever urge is
felt
Health educate on
the importance of
medication
.to allay anxiety.
To provide comfort.
To prevent urinary
retention and bladder
distention
To enable the patient
adhere to treatment
Void in sufficient
amounts with no
palpable bladder
distention.
Verbalize
understanding of
causative factors
and appropriate
interventions ,
Demonstrate
techniques/beha
viors to
alleviate/prevent
retention.
48.
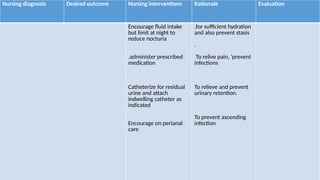
Nursing diagnosis Desiredoutcome Nursing interventions Rationale Evaluation
Encourage fluid intake
but limit at night to
reduce nocturia
.administer prescribed
medication
Catheterize for residual
urine and attach
indwelling catheter as
indicated
Encourage on perianal
care
.for sufficient hydration
and also prevent stasis
.
To relive pain, 'prevent
infections
To relieve and prevent
urinary retention.
To prevent ascending
infection
49.
Complications of benignprostate hyperplasia
• Urine retention. Urinary stasis happens as the enlarged prostate
blocks the bladder of excretion of urine
• Urinary tract infections. Due to the retention of urine in the bladder,
the environment becomes conducive for opportunistic bacteria to
proliferate thereby causing infection.
• Bladder stones. Because of incomplete excretion of urine waste will
continuously accumulate in the bladder thereby forming crystals that
may cause injury to the thin bladder walls.
50.
• Bladder damage.As the bladder can not properly empty, its muscles
weaken overtime. This loss in elasticity compromises its structure,
making contraction ineffective, thereby making urination difficult.
• Kidney damage. Increased pressure from urinary stasis and/ or
ascending infections from the bladder will reach the kidneys, thereby
causing damage overtime.
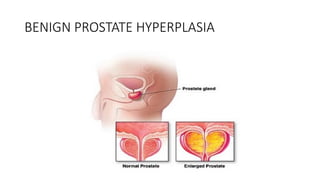
#9 The prostate gland enlarges, extending upward into the bladder and obstructing the outflow of urine.
#13 dysregulation of the insulin-like growth factor (IGF) axis has been implicated in the development of BPH and prostate cancer . The IGF axis regulates the physiologic and pathophysiologic growth of many organs including the prostate. insulin combines to IGF receptor to enter prostate cells, possibly causing receptor activation to induce growth and proliferation. Hyperinsulinemia is associated with lower levels of sex hormone-binding globulin, increasing the amount of sex hormone entering prostatic cells thereby influencing growth.
#20 HYDROnephrosis medical condition characterized by swelling or dilatation of one or both kidneys due to build up of urine.
#31 Upper urinary tract abnormalities that usually result from bladder outlet obstruction include upward displacement of the terminal portions of the ureters (fish hooking), ureteral dilation, and hydronephrosis.
#33 Effect of drugs is seen in 6months period. DHT is a male hormone that can build up in the prostate which may cause prostate growth. Side effects include erectile dysfunction, loss of libido
#35 About 10% of men undergoing TURP need the procedure repeated within 10 years because the prostate continues to grow.
#36 Erectile function and continence are usually retained, although about 5 to 10% of patients experience some acute postsurgical problems, most commonly retrograde ejaculation.



![• Other testing
Transrectal biopsy is usually done with ultrasound guidance (to
minimize risk of infection) and is usually indicated only if there is
suspicion of prostate cancer. Transrectal ultrasonography is an
accurate way to measure prostate volume.
Contrast imaging studies (eg, CT, intravenous urography [IVU]) are
rarely necessary unless the patient has had a urinary tract infection
(UTI) with fever or obstructive symptoms have been severe and
prolonged.](https://image.slidesharecdn.com/benignprostatehyperplesia-250312122653-3d0acaa9/85/BENIGN-PROSTATE-HYPERPLESIA-pptx-anatomy-and-physiology-30-320.jpg)

![• Pharmacologic Management
• Patients with mild to moderate obstructive symptoms, Alpha-
adrenergic blockers (eg. doxazosin, tamsulosin, alfuzosin, terazosin),
which relax the smooth muscle of the bladder neck and prostate may
decrease voiding problems.
• 5alpha reductase inhibitors. Hormonal manipulation with antiandrogen
agents (finasteride [Proscar],dutasteride) decreases the size of the
prostate and prevents the conversion of testosterone to
dihydrotestosterone (DHT).](https://image.slidesharecdn.com/benignprostatehyperplesia-250312122653-3d0acaa9/85/BENIGN-PROSTATE-HYPERPLESIA-pptx-anatomy-and-physiology-33-320.jpg)