Downloaded 348 times
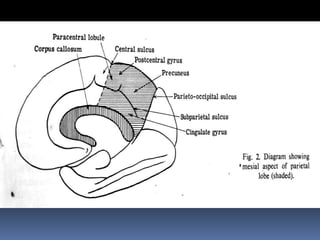



The parietal lobe is strategically located between other lobes and has a greater variety of clinical manifestations than other parts of the brain. It is involved in somatosensory processing, spatial awareness, language, praxis, and more. Damage can cause syndromes like Gerstmann syndrome, apraxia, agraphia, acalculia, hemispatial neglect, and others, depending on whether the left or right lobe is affected. The parietal lobe works in conjunction with other brain regions to carry out its diverse functions.