Downloaded 190 times



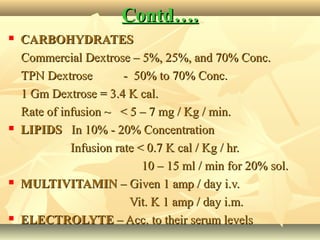
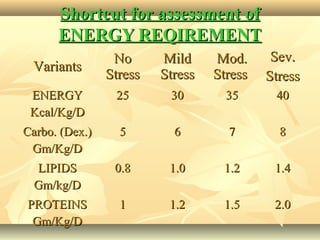
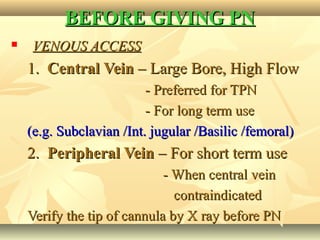





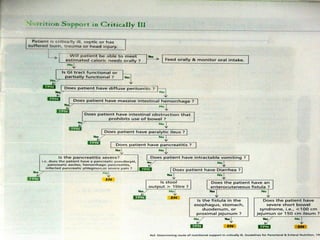



Parenteral nutrition, also known as total parenteral nutrition (TPN), involves intravenous administration of calories, nitrogen, and other nutrients to achieve tissue synthesis and anabolism when enteral nutrition is not possible or sufficient. It can be administered through either a central or peripheral vein. Proper assessment of a patient's malnutrition and nutrient requirements is important before starting parenteral nutrition to prevent complications and achieve optimal outcomes.



















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



