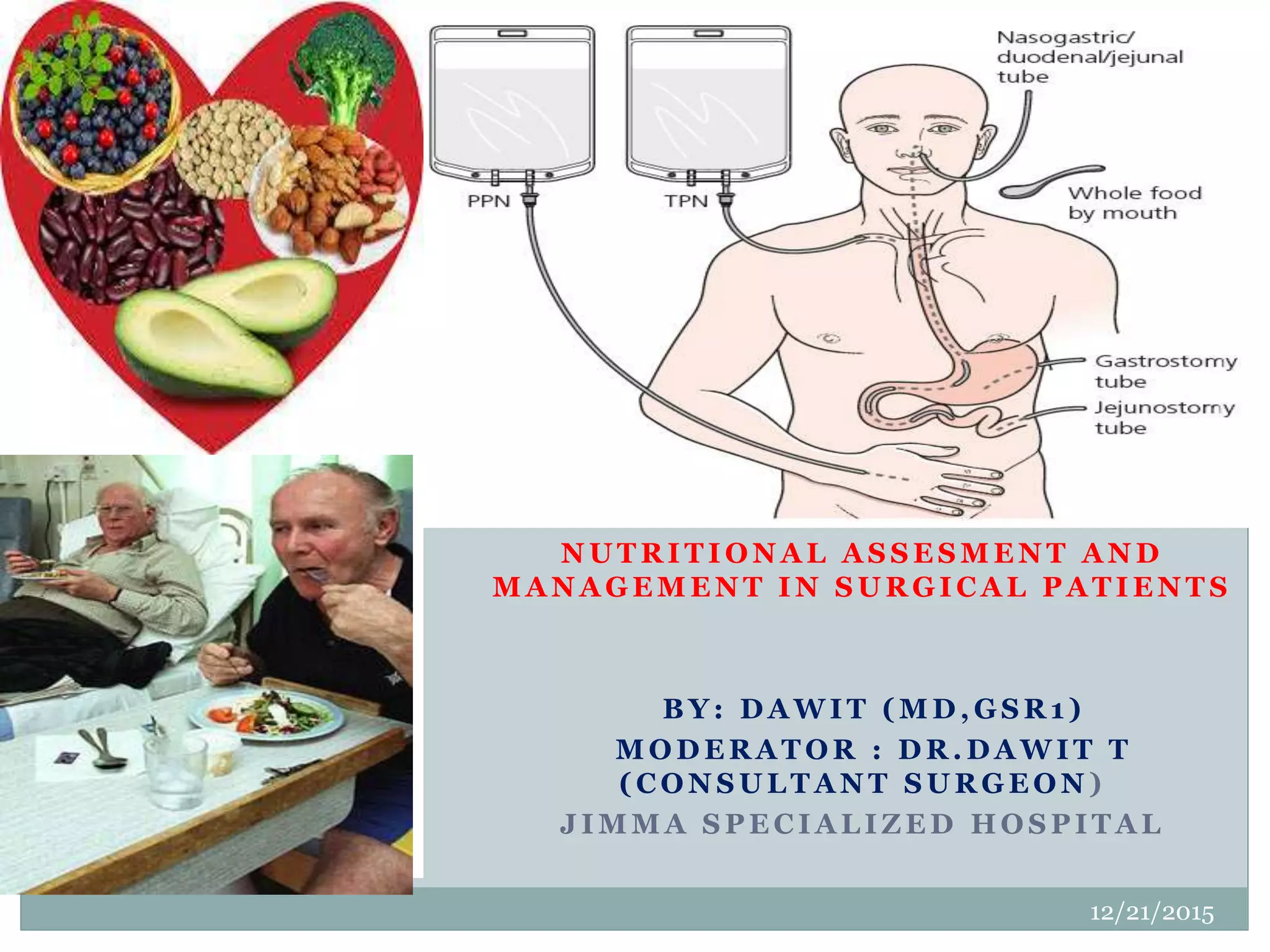
This document discusses nutritional assessment and management in surgical patients. It begins with an outline of the topics to be covered, including nutritional assessment, requirements, interventions, and disease-specific nutrition. Various methods of nutritional assessment are described, such as clinical history, physical exam, laboratory tests, and calculations of energy expenditure. Enteral and parenteral nutrition are presented as interventions, with details on their indications, delivery methods, and complications. The goal of nutritional support is to meet metabolic needs in patients who cannot maintain adequate intake orally.