Downloaded 1,729 times





















![Sentinel Lymph Node
• Sentinel lymph node (SLN):
• SLN biopsy was first clinically used for penile
carcinomas[2]
. Its utility in CA breast was explored in
a series of studies in the 1970s*.
• The first node in a regional lymphatic basin that
receives lymph flow from the primary tumor.
• The most lateral of the anterior group of lymph
nodes (level I) is the usual site of SLN in CA breast.
• SLN biopsy is indicated in patients with clinically node
negative disease.
* Pieter J Tanis. Breast Cancer Research. 2001](https://image.slidesharecdn.com/breastanatomy-170524174925/75/Breast-anatomy-37-2048.jpg)
![SLN Biopsy
• Localize tumor
• Dermal injection (raise a wheal) of radiocolloid into skin
overlying tumor in 5 locations
• 0.5 mCi Tc sulphur colloid in 0.5cc. After ~1 hour, take
patient to the OR.
• 5 cc of dye is injected, typically isosulfan blue, followed by
massaging for 5 minutes. Methylene blue can also be used.
• Subareolar injection (into Sappey’s plexus) is the best.
• The combination of radioisotope and dye provides the most
accurate means of localizing the sentinel node.[12]](https://image.slidesharecdn.com/breastanatomy-170524174925/75/Breast-anatomy-38-2048.jpg)












![Breast & Chest wall Contours: Anatomical Boundaries
[13]
Cranial Caudal Ant Posterior Lateral Medial
Breast Clinical
reference +
2nd rib
insertion
Clinical
reference +
Loss of CT
apparent
breast
Skin Excludes
Pectoralis
chest wall
muscles, &
ribs
Clinical
reference +
mid axillary
line typically,
excludes Lat.
dorsi
Sternal-rib
junction
Breast +
chest
wall
Same Same Same Includes
pectoralis,
chest wall,
ribs
Same Same
Chest
wall
Caudal
border of
the clavicle
head
Clinical
reference +
loss of CT
apparent
breast
Skin Rib-pleural
interface
(includes
pectoralis,
chestwall
muscles, ribs)
Clinical
reference/mi
d axillary line
typically,
excludes Lat.
dorsi
Sternal rib
junction](https://image.slidesharecdn.com/breastanatomy-170524174925/75/Breast-anatomy-51-2048.jpg)






![Cranial Caudal Anterior Posterior Lateral Medial
Supra
Clavivular
Caudal to
cricoid
Junction of
brachio
cephalic veins
/ caudal edge
clavicle head
Sterno-
mastoid
(SCM)
Ant
aspect of
Scalene
Cranial: lat
edge SCM
Caudal:
Junction 1st
rib-clavicle
Exclude
thyroid
and
trachea
Axillary
Level I
Axillary
vessels cross
lat edge of
pect minor
Pectoralis
major insert.
Into ribs
Plane
defined by
ant surface
of pec
major + Lat
dorsi
Ant
surface of
sub-
scapularis
Medial border
of Lat dorsi
Lateral
border
Pec minor
Axillary
Level II
Axilarry
vessels cross
medial edge
of pect minor
Axillary
vessels cross
lat edge of
Pec minor
Ant surface
Pec minor
Ribs and
inter-
costal
muscles
Lat border
Pec minor
Medial
border
Pec minor
Axillary
Level III
Pect minor
insert. on
cricoid
Axillary
vessels cross
medial edge
Pec minor
Post
surface
Pect major
Ribs and
inter-
costals
Medial border
Pect minor
Thoracic
inlet
Internal
mammary
Superior aspect
medial 1st rib
Cranial aspect
of 4th rib
- - - -
Regional Node Contours: Anatomical Boundaries
[13]](https://image.slidesharecdn.com/breastanatomy-170524174925/75/Breast-anatomy-58-2048.jpg)

































![MRI of Breast
• A recent meta-analysis of 44 studies has estimated the
sensitivity and specificity of MRI for the diagnosis of
breast cancer as 90% & 72%.[10]
• It is particularly useful in
• Dense breasts
• Palpable abnormality with normal mammogram
• Augmented breasts
• To stage a tumor (eg chest wall invasion)](https://image.slidesharecdn.com/breastanatomy-170524174925/75/Breast-anatomy-92-2048.jpg)





![Molecular Breast Imaging
• New Technique using targeted molecules (eg. FES for the
estrogen receptor).
• Has been shown to be a good complementary technique to
conventional mammography, especially for women with a
dense breast.[4, 5]
• Especially useful for imaging patients who cannot have an
MRI.[6]
• More cost effective and less time consuming than MRI.[6,7]](https://image.slidesharecdn.com/breastanatomy-170524174925/75/Breast-anatomy-98-2048.jpg)


![Digital Breast Tomosynthesis
• Developed to improve detection and characterization of
breast lesions especially in women with dense breasts
• In this technique, multiple projection images are
reconstructed allowing visual review of thin breast
sections.
• Potential to unmask cancers obscured by normal tissue
located above and below the lesion, but no randomized
evidence of advantage over mammograms yet.[8]](https://image.slidesharecdn.com/breastanatomy-170524174925/75/Breast-anatomy-101-2048.jpg)



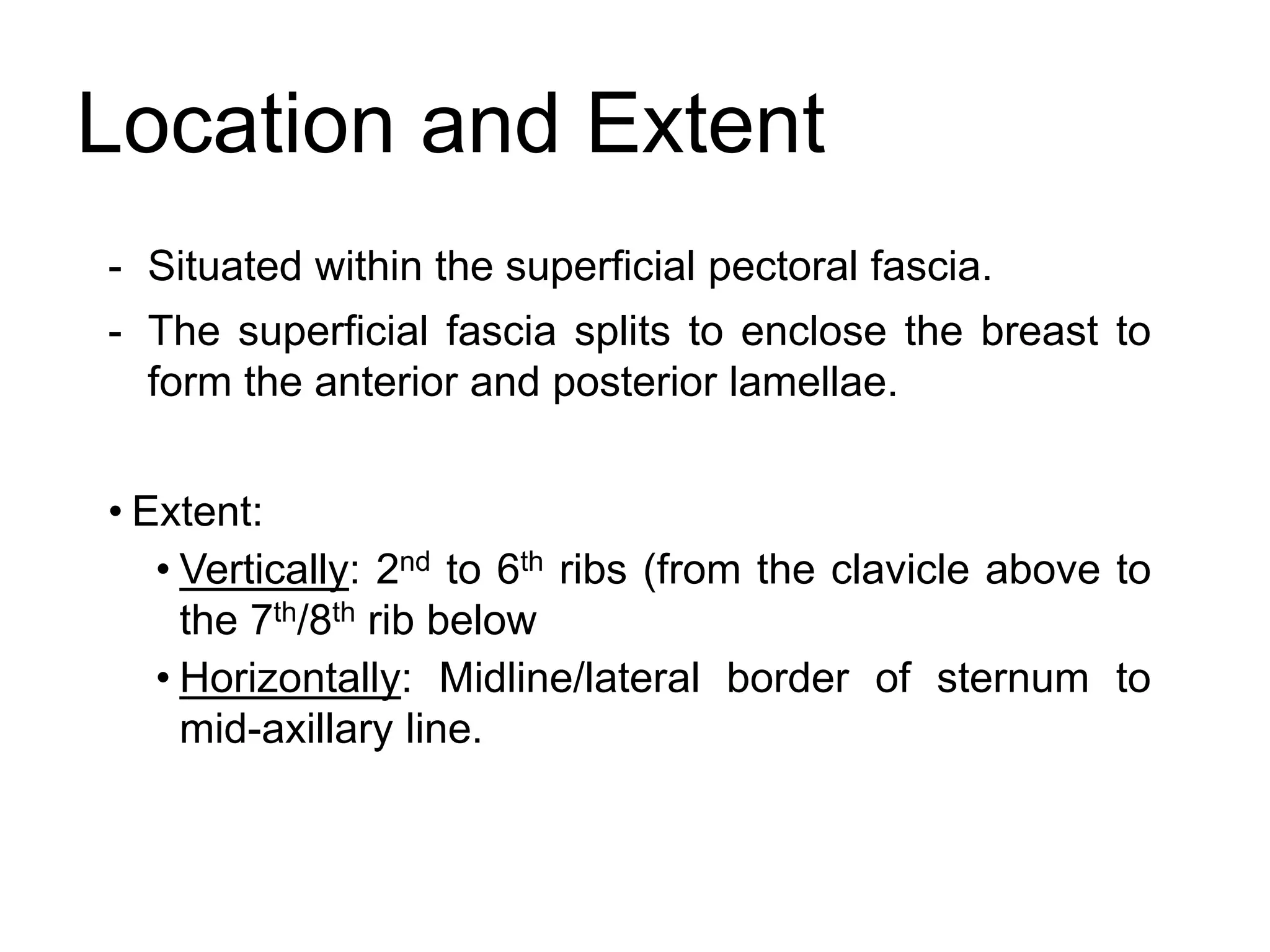
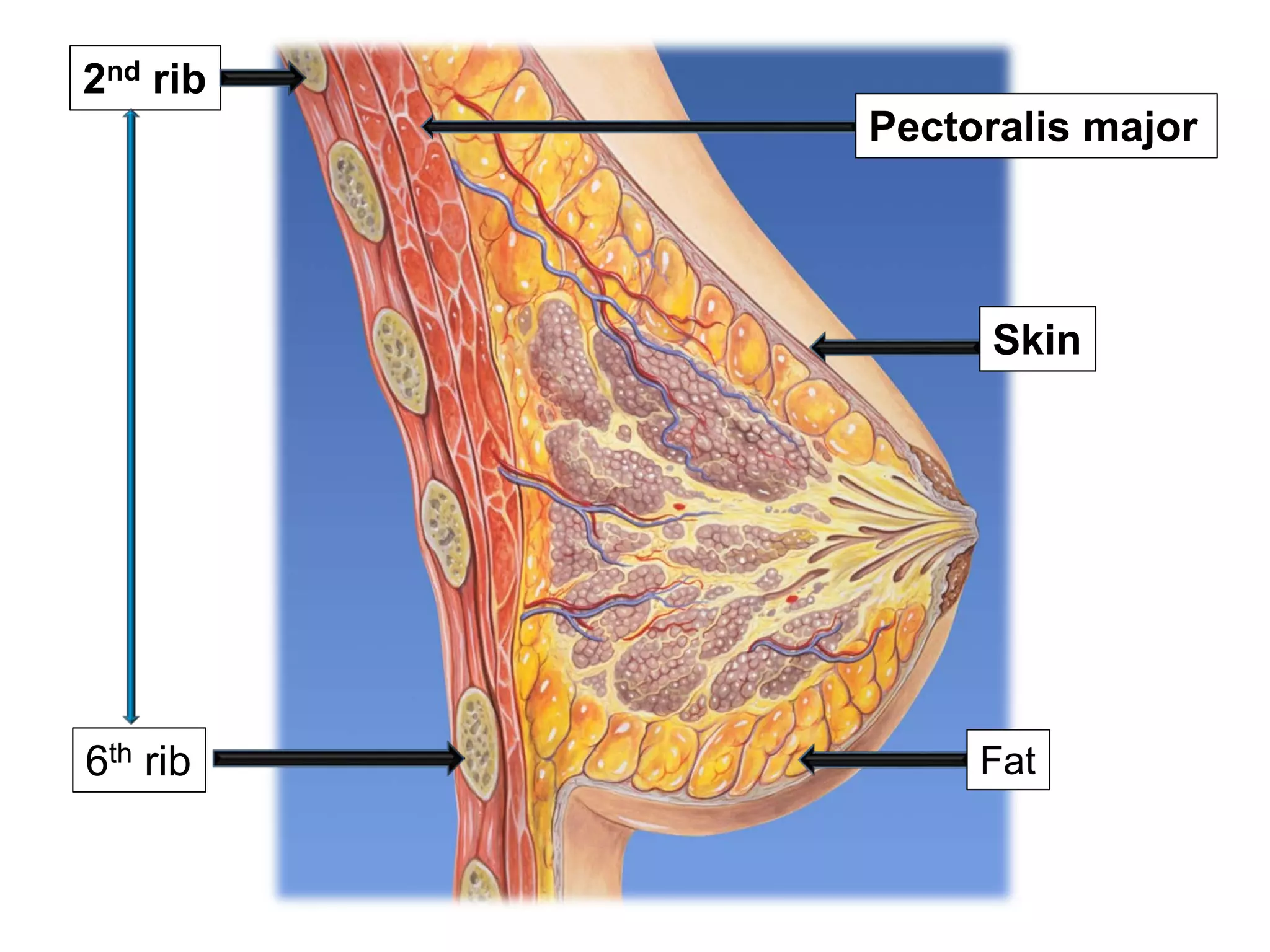
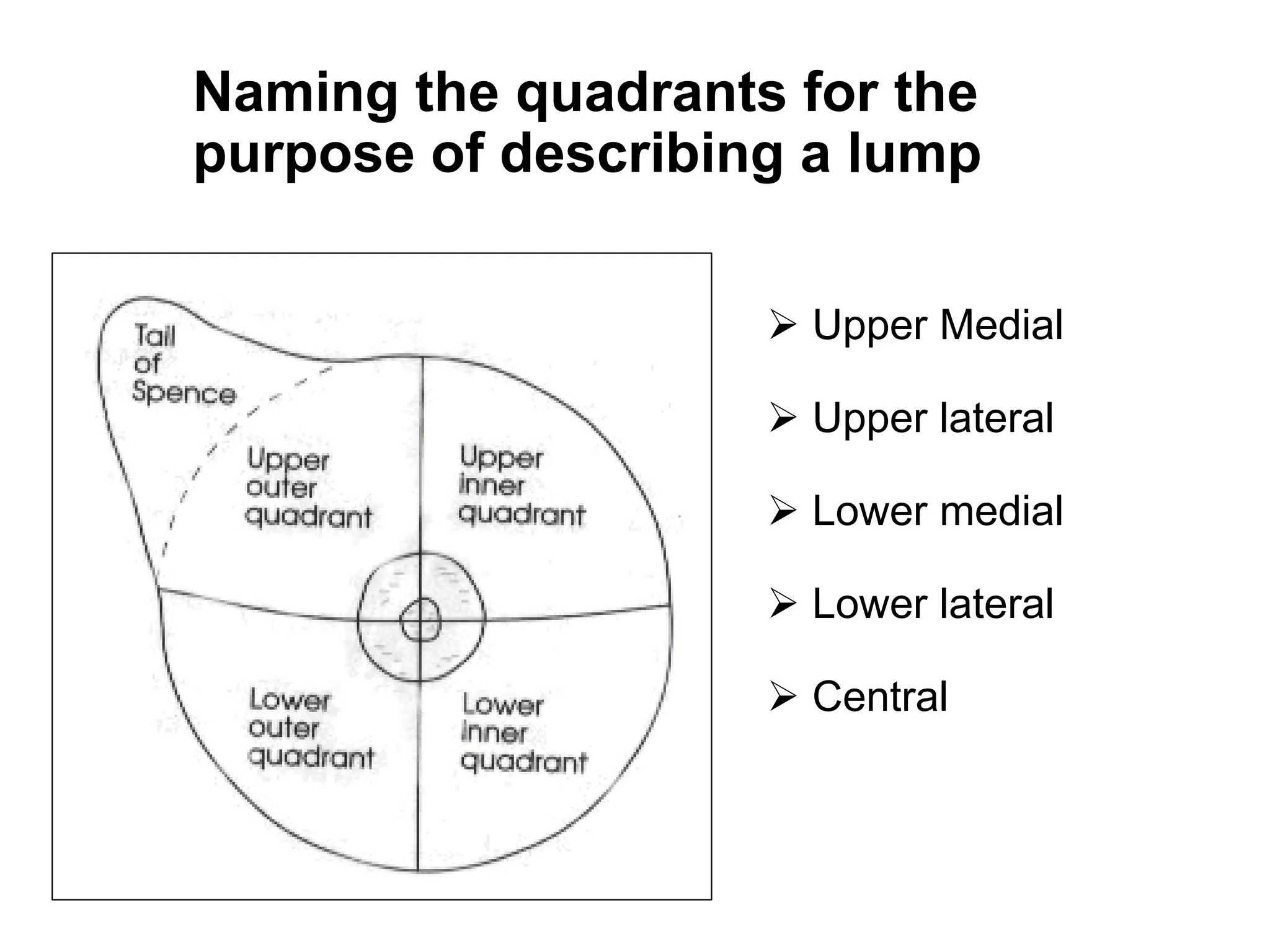
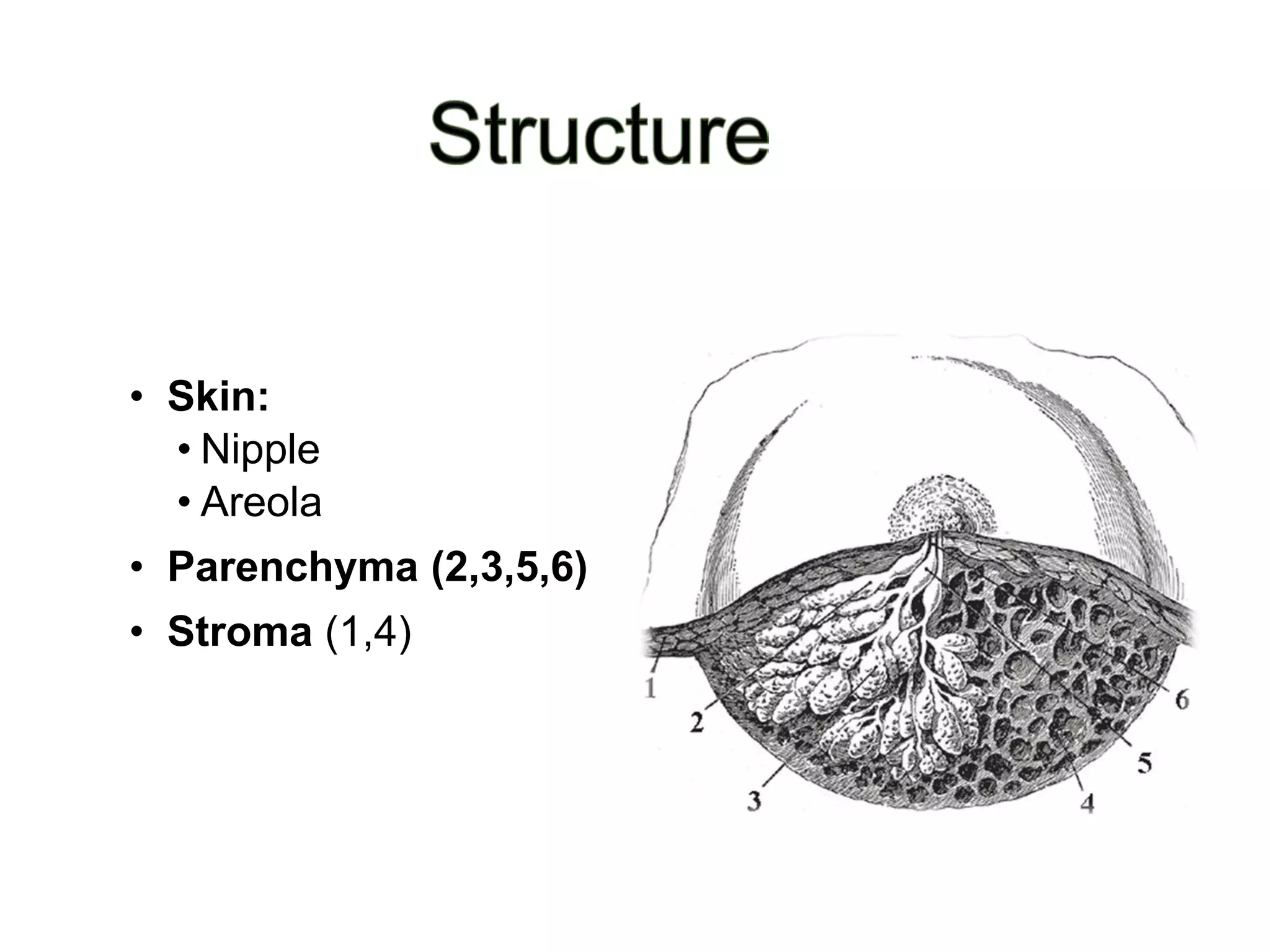
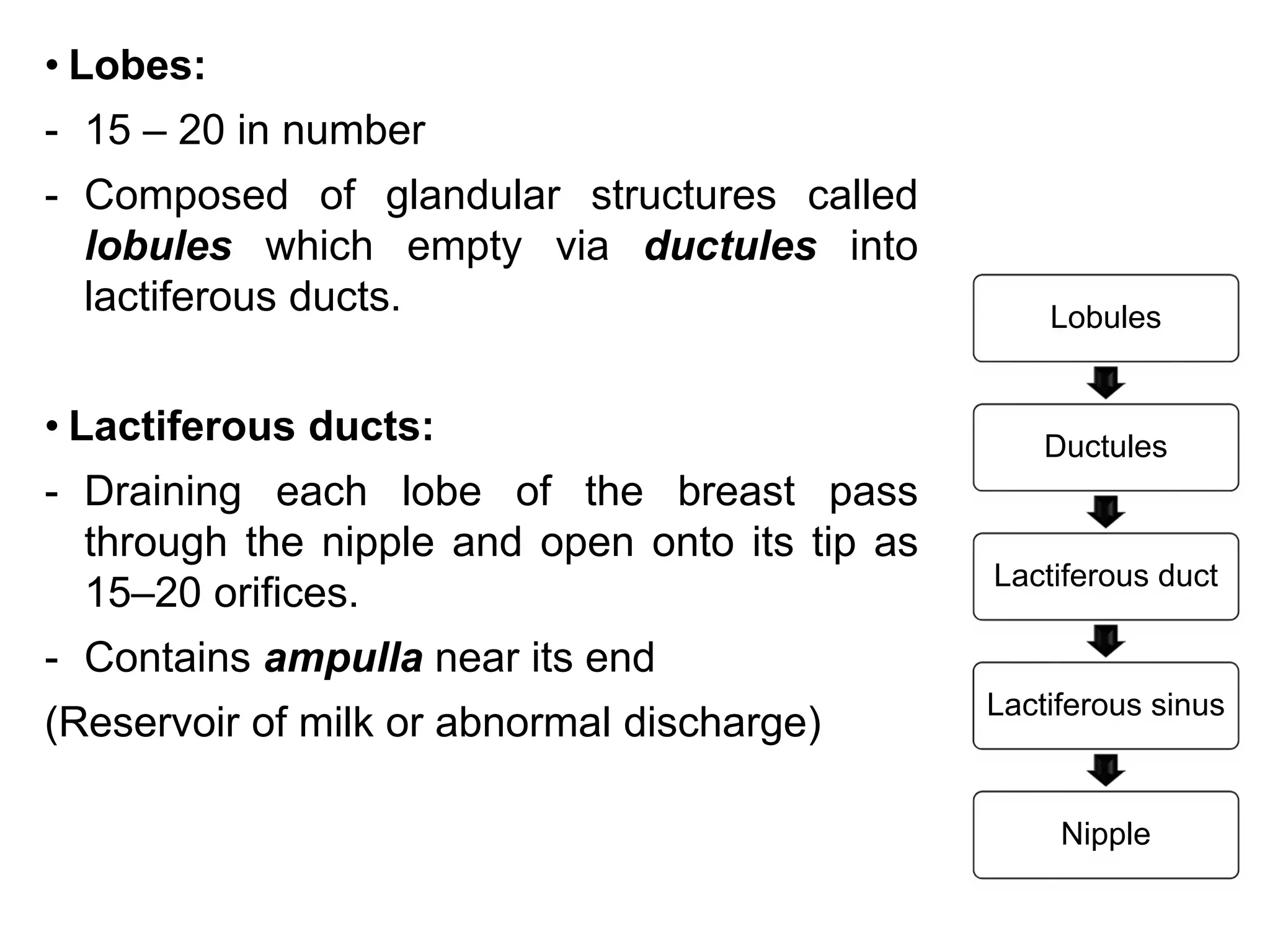
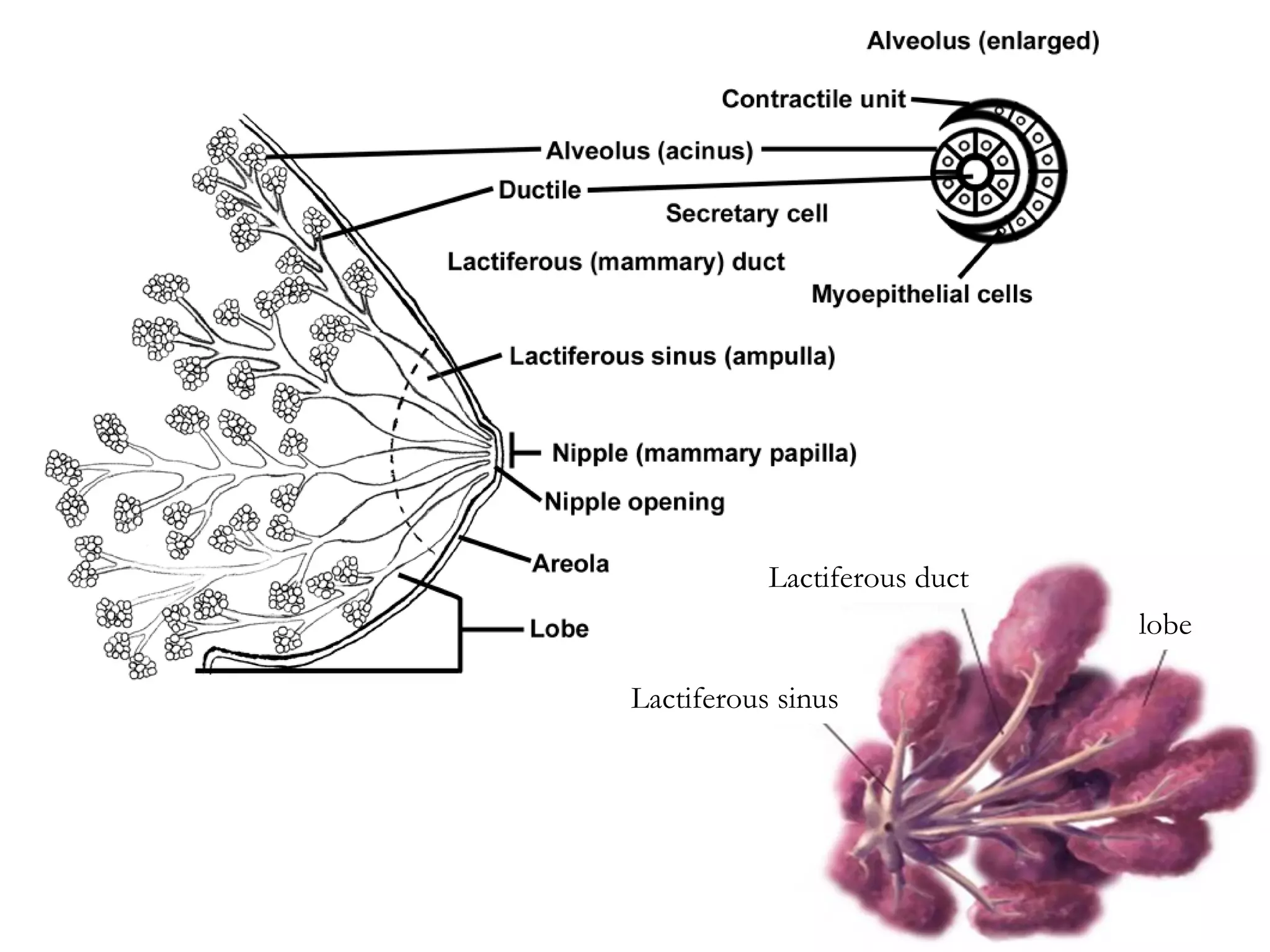
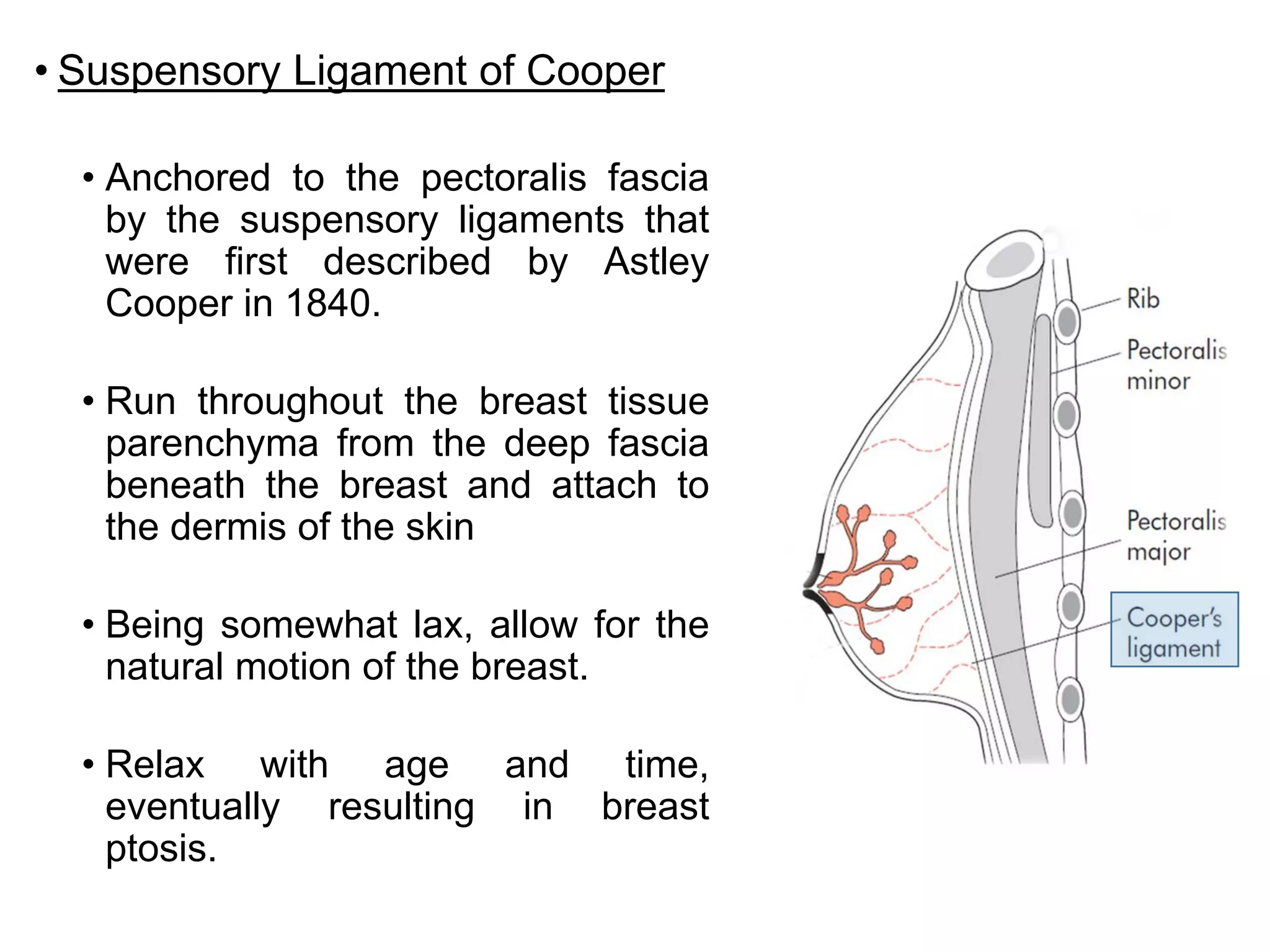
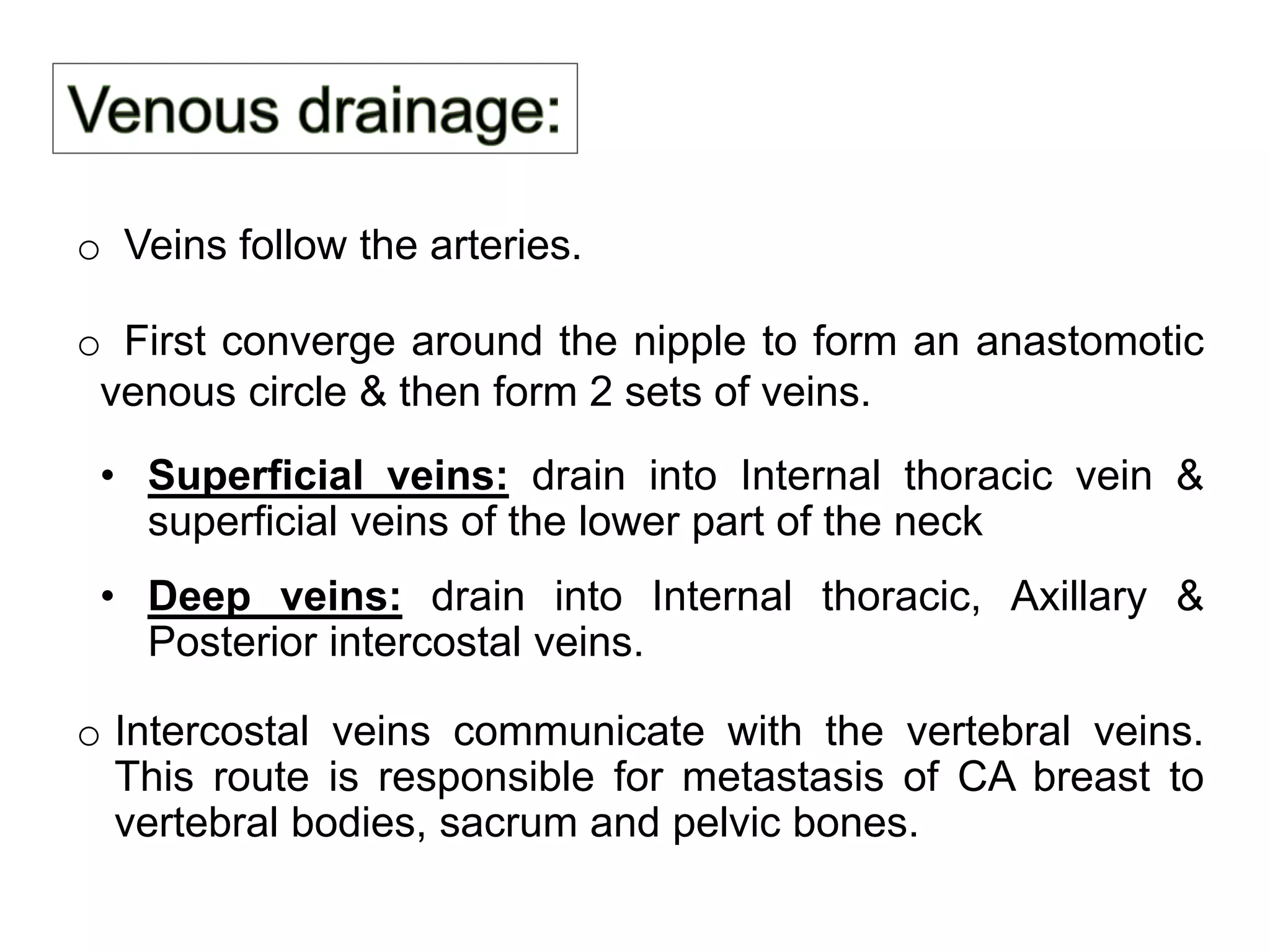
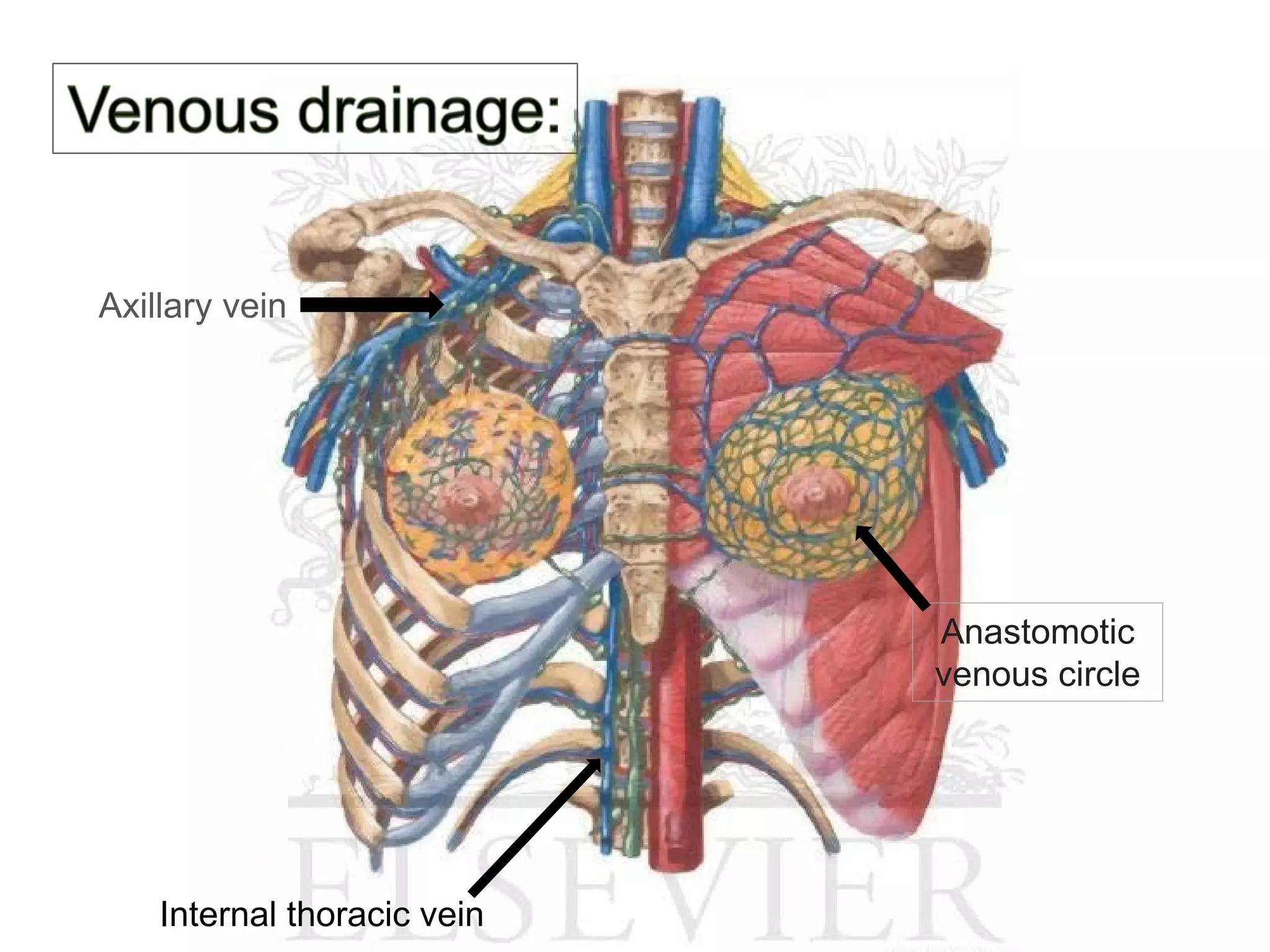
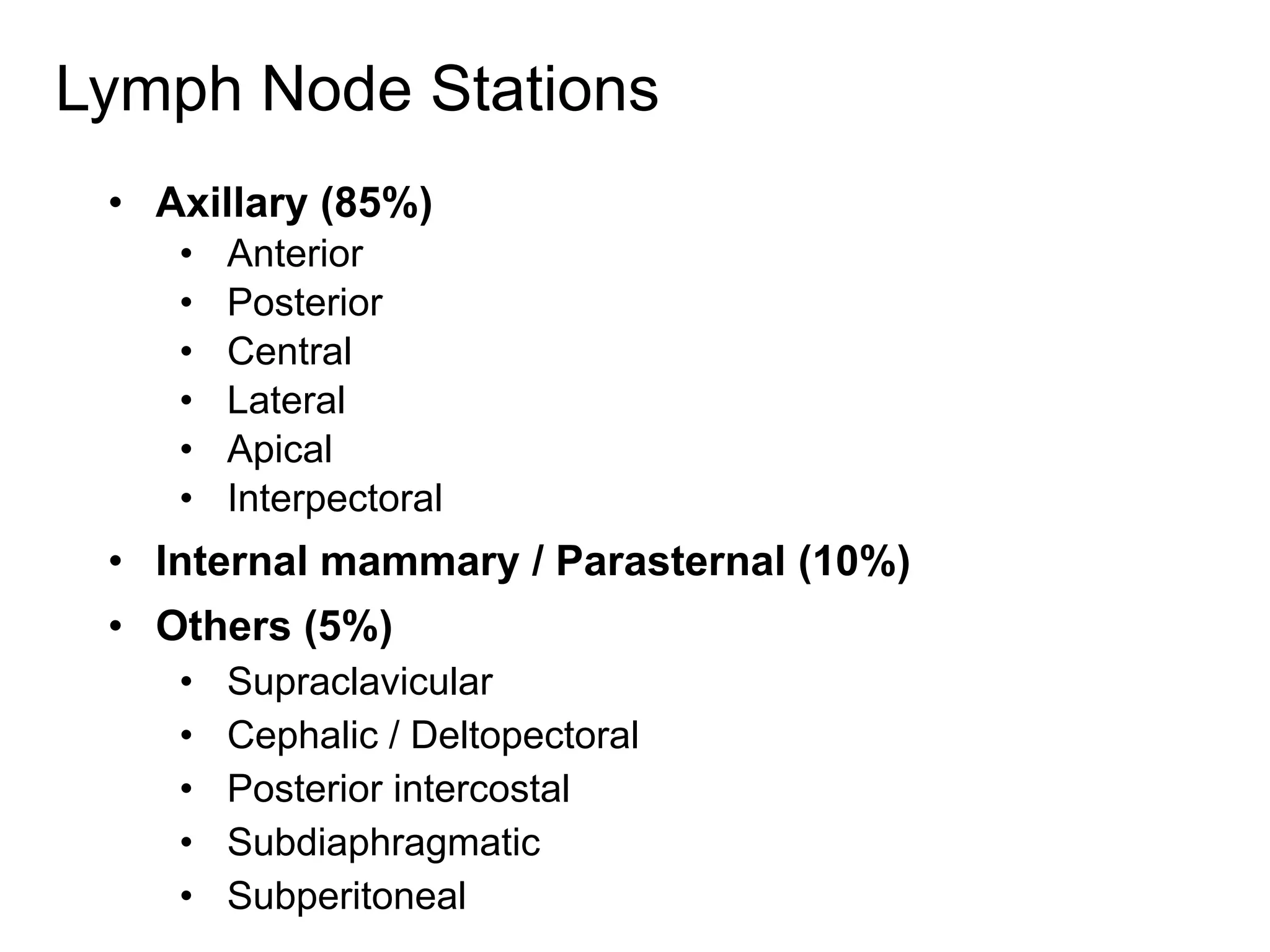
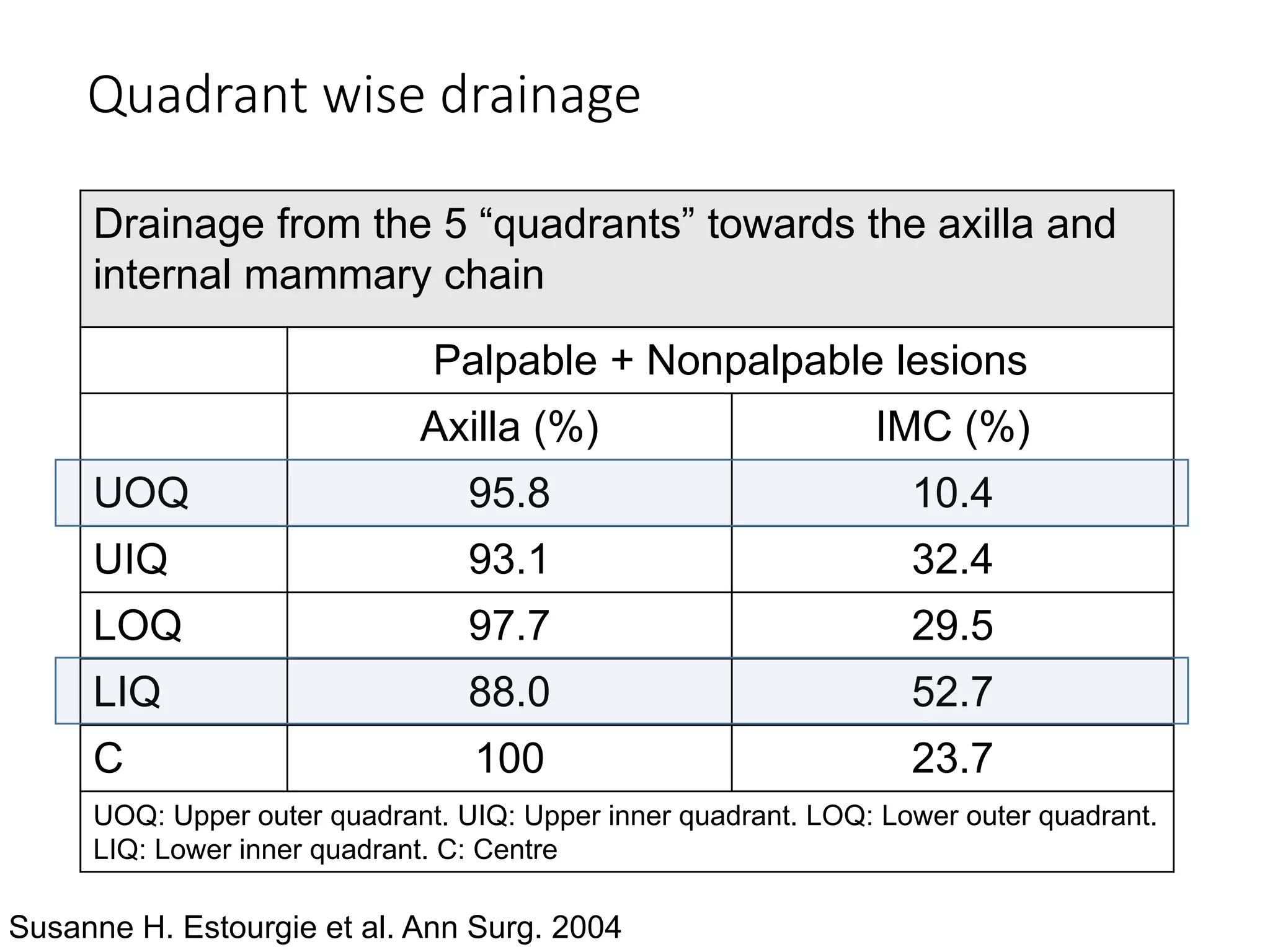
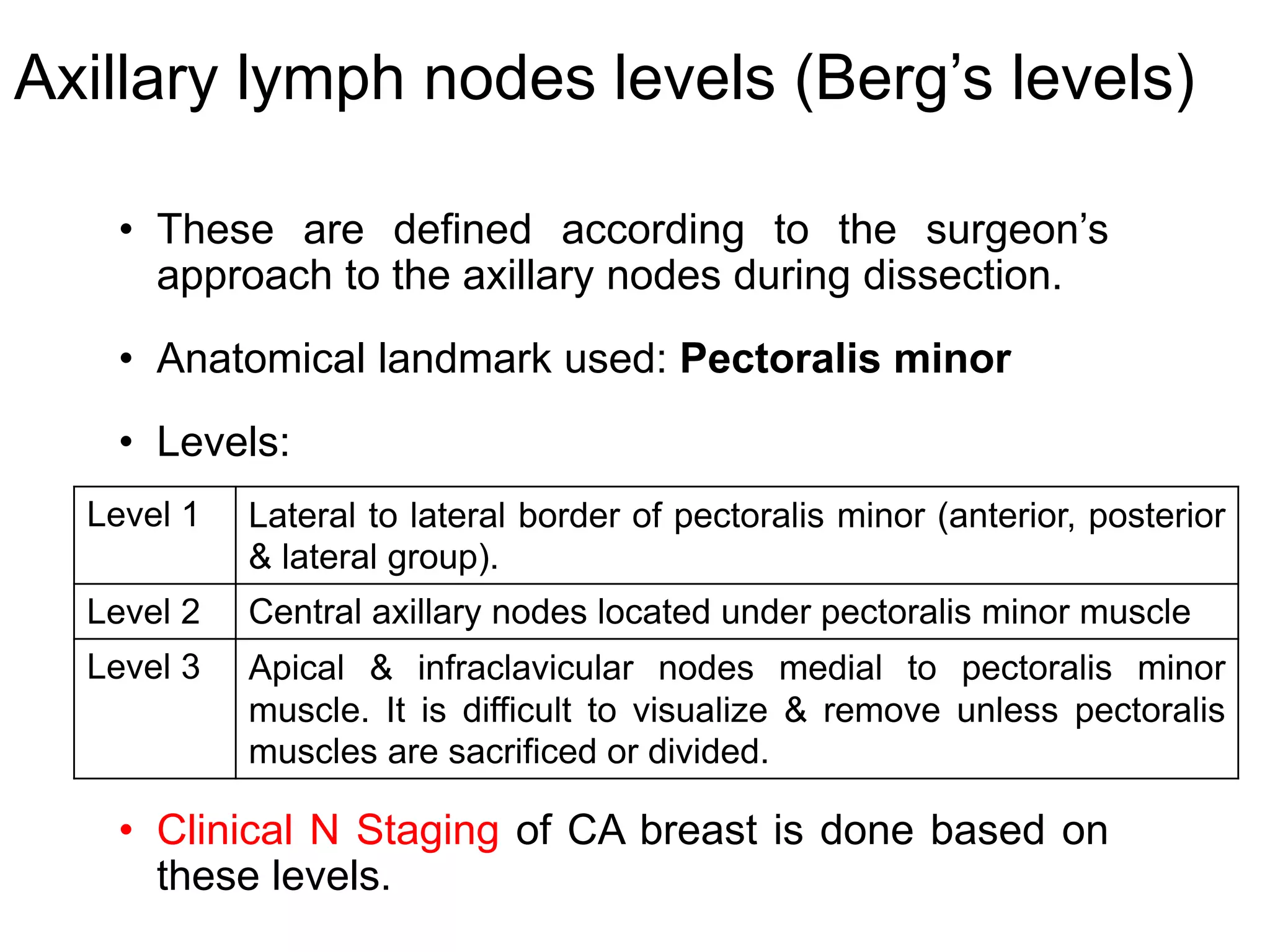
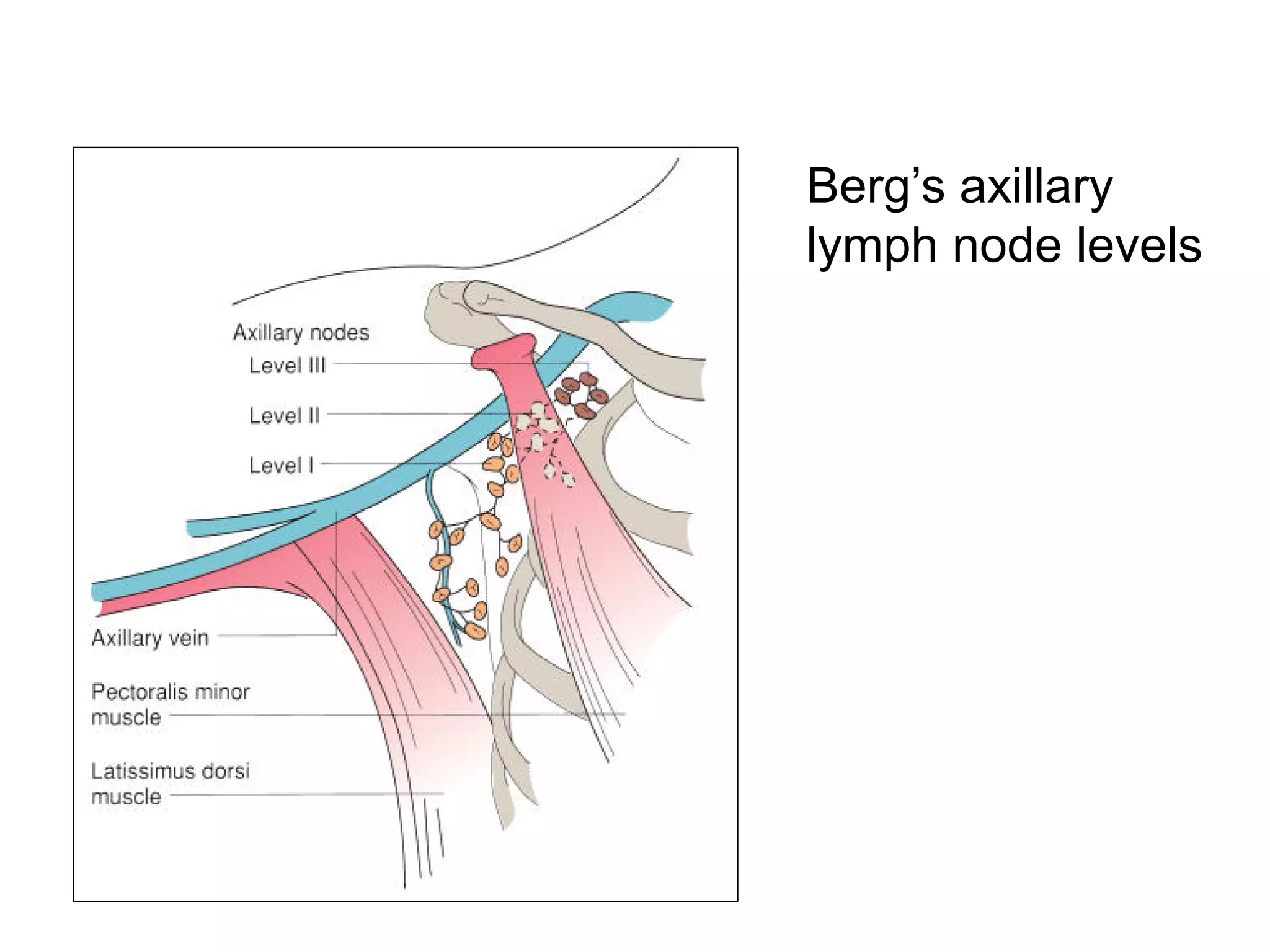
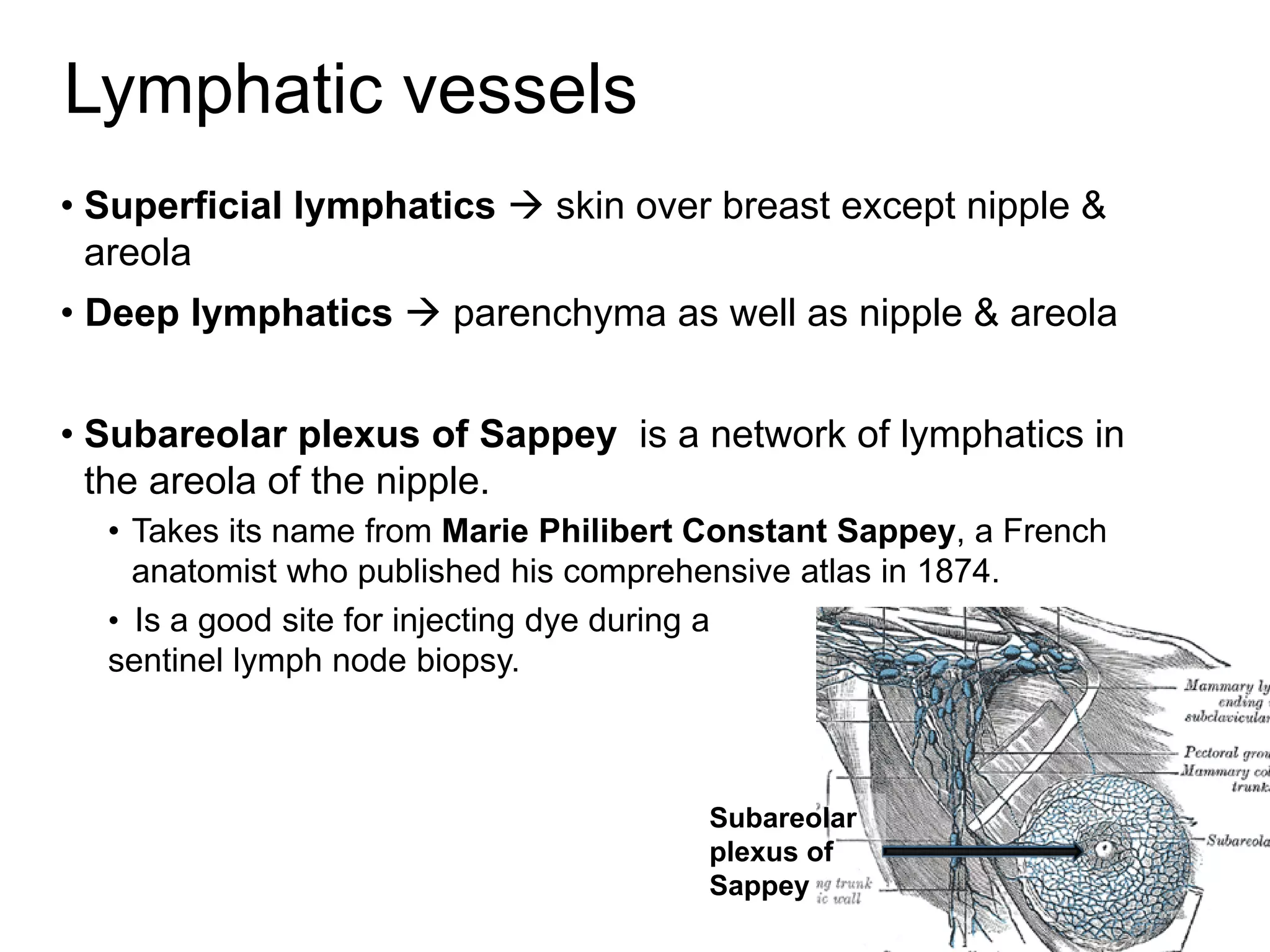
The document discusses the anatomy of the breast. It covers topics such as location and extent of the breast, layers and structures within the breast like skin, parenchyma, ducts and lobes. It also discusses blood supply, lymphatic drainage including lymph node stations, nerve supply and radiological anatomy of the breast.