Diagnosis and SuspectedCause
◦5. Suspected Condition: Primary
hyperparathyroidism.
6. Possible Cause: Parathyroid adenoma as
revealed by an ultrasound showing an
enlarged parathyroid gland.
5.
LEARNING OBJECTIVES:
◦ 1_ANATOMYOF PARATHYROID GLAND
◦ 2_DEVELOPMENT OF PARATHYROID GLAND
◦ 3_MICROSCOPIC ANATOMY OF PARATHYROID GLAND
◦ 4_PATHOPHYSIOLOGY OF PRIMARY HYPERPARATHYROIDISM
◦ 5_TYPES OF PRIMARY HYPERPARATHYROIDISM
◦ 6_SYMPTOMS
◦ 7_CAUSES
◦ 8_LAB INVESTIGATIONS
◦ 9_MANAGEMENT STRATEGIES
6.
ANATOMY OF PARATHYROID
GLAND:
.Location:
- Usually 4 small glands(can be 2–6)
- Located on the posterior surface of the thyroid gland
Divided into:
- 2 superior parathyroid glands
- 2 inferior parathyroid glands
7.
*
2. Size &Shape:
Small, oval or bean-shaped
Size: ~6 mm long, 3–4 mm wide
Weight: ~30–50 mg each
3. Blood Supply:
- Arterial supply:
- Mainly from the inferior thyroid artery
- May also get branches from superior thyroid artery or
thyroid ima artery
3- Venous drainage:
- Into the thyroid venous plexus
4. Nerve Supply:
- From sympathetic fibers via cervical ganglia
◦- No parasympathetic innervation
8.
DEVELOPMENT OF PARATHYROID
GLAND:
Theparathyroid glands develop from the epithelium of the
pharyngeal (branchial) pouches, specifically:
Origin:
3rd
Pharyngeal Pouch → Inferior Parathyroid Glands
4th
Pharyngeal Pouch → Superior Parathyroid Glands
9.
◦Developmental Process:
Structure Derivative
3rd
PharyngealPouch
Dorsal part → Inferior parathyroid glands
Ventral part → Thymus
4th
Pharyngeal Pouch
Dorsal part → Superior parathyroid glands
Ventral part → Ultimobranchial body (forms C-cells
of thyroid)
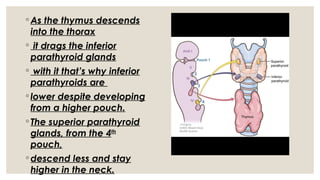
10.
◦ As thethymus descends
into the thorax
◦ it drags the inferior
parathyroid glands
◦ with it that’s why inferior
parathyroids are
◦ lower despite developing
from a higher pouch.
◦ The superior parathyroid
glands, from the 4th
pouch,
◦ descend less and stay
higher in the neck.
◦ Oxyphil Cells
◦
◦- Appear around puberty; number increases with age
◦ - Larger than chief cells, roughly polygonal
◦ - Occur in small clusters
◦ - Intensely acidophilic staining due to numerous
mitochondria
- No secretory granules present; function unknown
13.
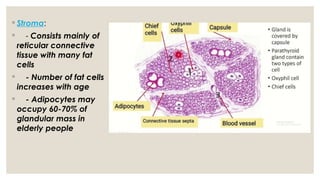
◦ Stroma:
◦ -Consists mainly of
reticular connective
tissue with many fat
cells
◦ - Number of fat cells
increases with age
◦ - Adipocytes may
occupy 60-70% of
glandular mass in
elderly people
14.
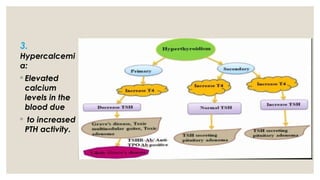
Pathophysiology of primary
hyperthyroidism:
Parathyroidgland dysfunction:
◦Adenoma, hyperplasia, or carcinoma leads to
excessive parathyroid hormone (PTH) production
◦ Increased PTH secretion:
◦Elevated PTH levels stimulate:
◦ - Bone resorption (calcium release from bones)
◦ - Increased calcium absorption in the gut
◦ - Enhanced calcium reabsorption in the
kidneys.
Causes:
1.Parathyroid Adenoma: Abenign tumor on one of
the parathyroid glands, leading to excessive
parathyroid hormone (PTH) production.
2. Parathyroid Hyperplasia: Enlargement of multiple
parathyroid glands, resulting in overproduction of PTH.
3.Parathyroid Carcinoma:A rare malignant tumor of
the parathyroid gland that can cause excessive PTH
production.
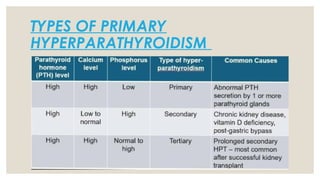
18.
SYMPTOMS:
1. Bone painor tenderness
2. Kidney stones
3. Fatigue
4. Depression
5. Abdominal pain
6. Constipation
7. Frequent urination
8. Thirst
Asymptomatic Cases
Some individuals may not experience noticeable symptoms, and the condition is
discovered during routine blood tests.
Complications
Untreated primary hyperparathyroidism can lead to complications
such as osteoporosis, kidney damage, and cardiovascular disease.
5. 24-hour UrinaryCalcium:
- *↑ Increased* (to assess calcium excretion)
6. Vitamin D Levels:
- May be low or normal
7. Bone Mineral Density (DEXA scan):
- Shows bone loss (osteopenia or osteoporosis)
8. Neck Ultrasound:
- To detect parathyroid adenoma or hyperplasia
21.
Management strategies:
◦Surgical treatments:
◦1) Minimally invasive parathyroidectomy:
◦ • Favored when only one gland is affected.
◦
◦ 2) Bilateral Neck Exploration:
• Used when multiple glands are involved, or when the
location of the adenoma is not clearly identified with
imaging.
22.
Medical Management:
t
🔹 Cinacalcetsecretion
• Reduces serum calcium levels
🔹 Bisphosphonates (e.g., Alendronate)
• Inhibit bone resorption → increase bone mineral density
• Do not lower serum calcium or PTH
🔹 Hydration
• Encouraged to prevent kidney stones
• Avoid thiazide diuretics (they increase calcium levels)
23.
Monitoring (in asymptomaticpatients)
• Serum calcium and creatinine: annually
• Bone mineral density: every 1–2 years
• 24-hour urinary calcium (to assess stone
risk)
◦• Maintaining calcium and vitamin D levels