Downloaded 91 times

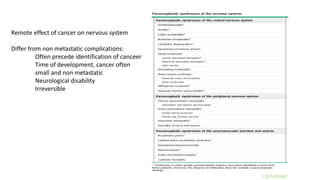
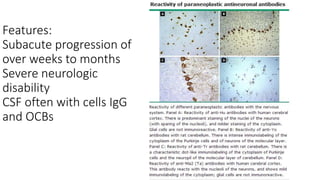




This document discusses neurological paraneoplastic syndrome, a heterogeneous group of neurological disorders caused by an immune response to cancer rather than directly from the cancer or its treatment. Key points: - The immune system mounts an abnormal response against antigens expressed by the cancer that are similar to neuronal antigens, leading to damage of nerve or muscle tissue. - Symptoms can include problems in the cerebral cortex, neuromuscular junction, or multiple areas of the nervous system. Neurological disability is often severe and irreversible. - Diagnosis involves identifying well-characterized antibodies, detecting cancer within 5 years, and ruling out other causes. Screening cancer patients without neurological symptoms still occasionally finds paraneoplastic antibodies.






















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
