Downloaded 164 times





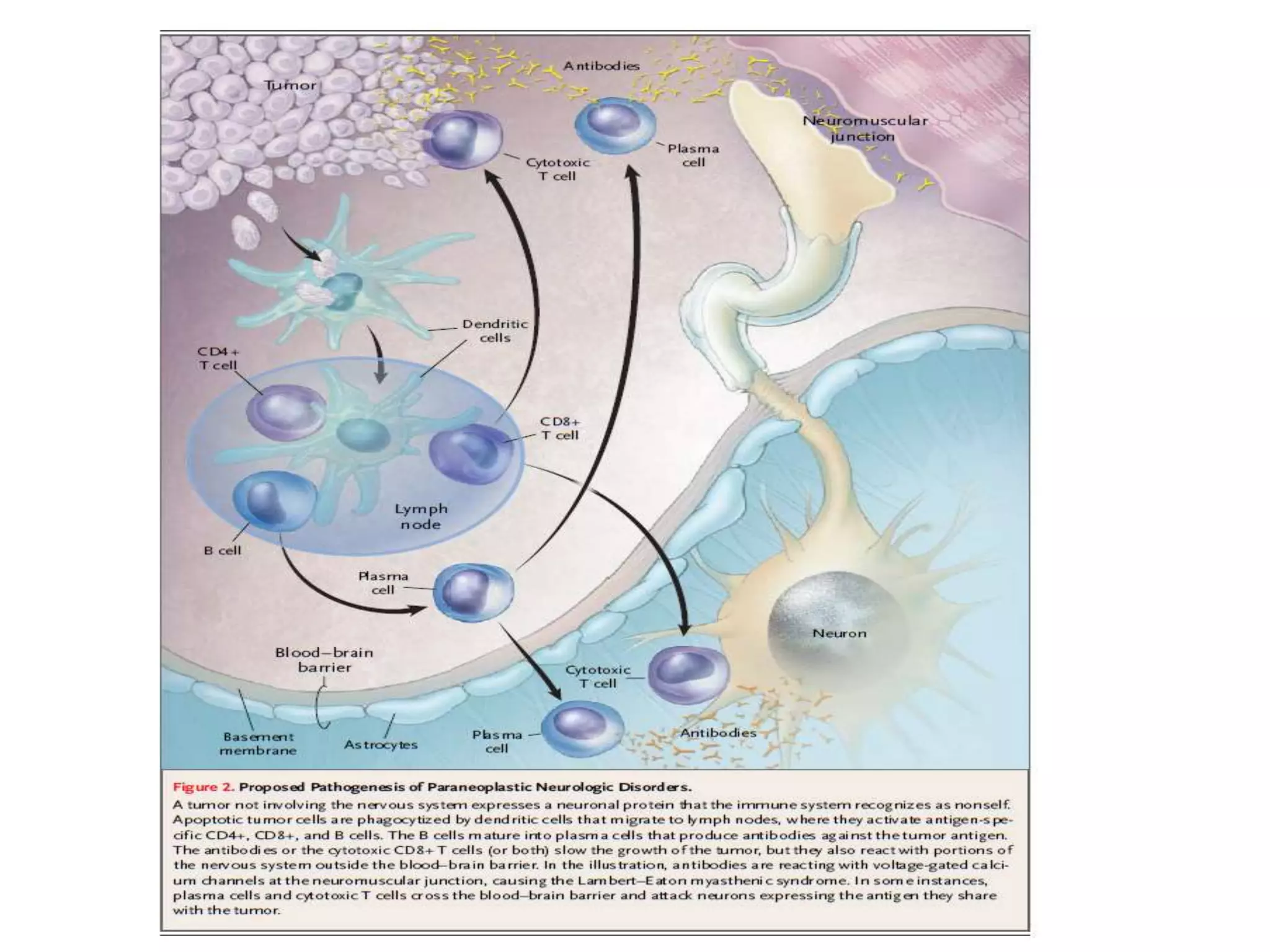


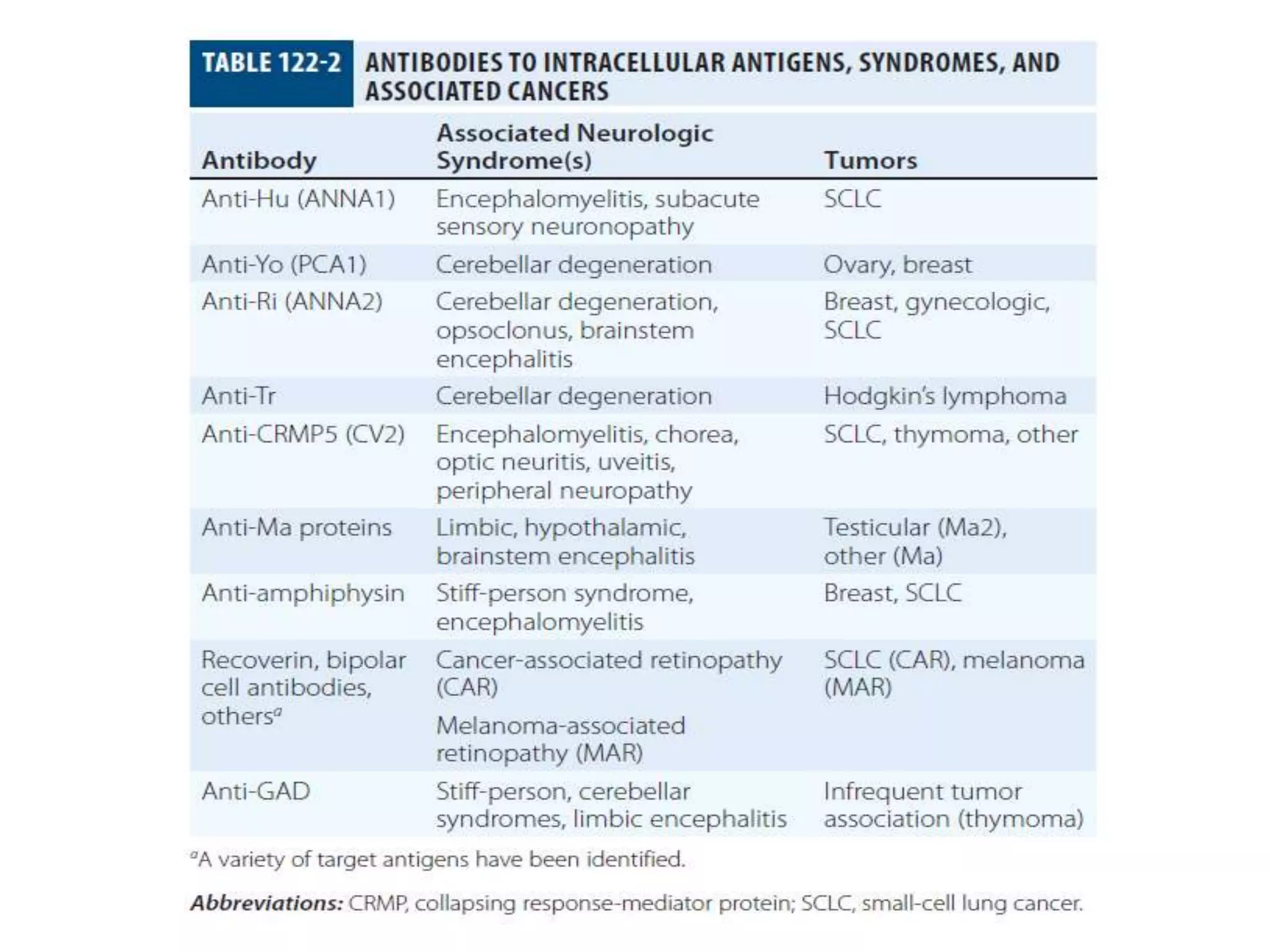

















The document is a comprehensive guide on paraneoplastic syndromes (PNS), detailing their definitions, pathogenesis, classifications, and examples of both classical and non-classical syndromes associated with various cancers. It highlights the immune system's involvement in the development of PNS and the neurological symptoms that may arise as a result, emphasizing that prompt detection and treatment of underlying tumors can improve outcomes. The guide covers specific syndromes such as encephalomyelitis, cerebellar degeneration, and visual syndromes, along with their associated tumors and suggested treatments.




















































































