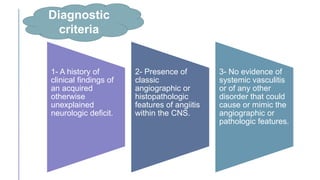
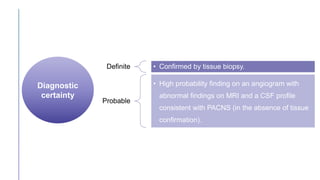
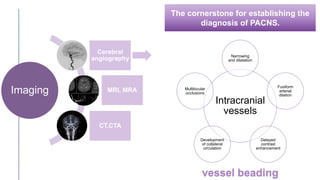
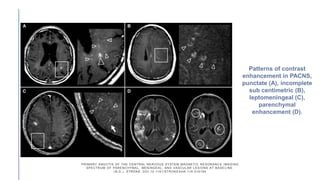
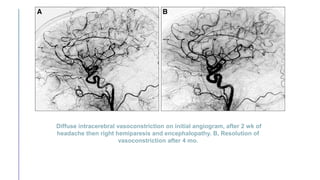
Primary central nervous system vasculitis (PACNS) is a rare disorder characterized by inflammation of blood vessels in the brain and spinal cord. It presents with non-specific symptoms like headache, cognitive impairment, and focal neurological deficits. Diagnosis involves neuroimaging showing multifocal lesions, angiography revealing vessel narrowing and dilation, and brain biopsy detecting immune cell infiltration of vessel walls. While the cause is unknown, infectious agents may trigger PACNS. Treatment involves immunosuppression but prognosis depends on disease severity and response to treatment.











![Myelin Oligodendrocyte Glycoprotein (MOG) Antibody Disease [MOG-AD]](https://cdn.slidesharecdn.com/ss_thumbnails/myelinoligodendrocyteglycoproteinmogantibodydisease0920-200920055159-thumbnail.jpg?width=640&height=640&fit=bounds)









































































