Downloaded 136 times
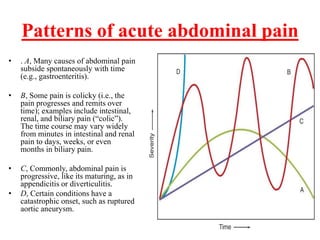
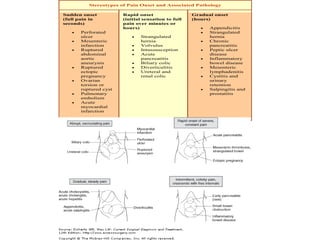
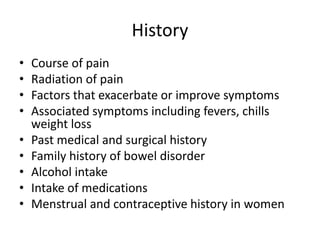
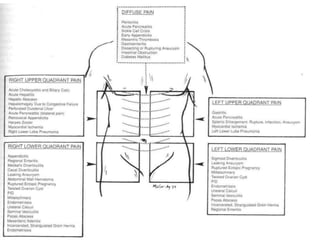




- Abdominal pain has many potential causes and determining the origin requires a detailed history, physical exam, and sometimes diagnostic tests. - The location, character, timing and associated symptoms of the pain provide clues to its underlying mechanism, such as inflammation, obstruction, vascular or nerve issues. - A thorough physical exam including inspection, abdominal palpation, and assessment of vital signs can help identify conditions like peritonitis but may not reveal the specific cause.






























































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)










![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

