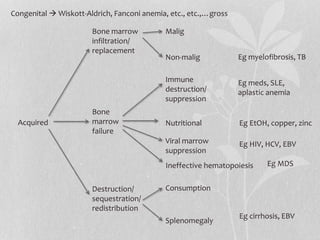
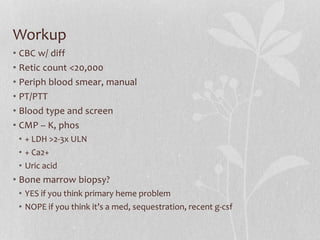
This document contains an agenda and summary for a noon conference on bone marrow failure. The agenda includes discussing the pathogenesis, basic workup, additional tests that were done for a patient, and taking questions. The pathogenesis section outlines different causes of bone marrow failure including congenital issues, acquired issues, bone marrow infiltration/replacement, destruction/sequestration/redistribution, consumption, and ineffective hematopoiesis. The basic workup section lists various blood tests that should be considered. Additional tests that were done for their patient are also listed.


























































![2019 04-30 noon conference [stephen slade]](https://cdn.slidesharecdn.com/ss_thumbnails/2019-04-30noonconferencestephenslade-190501212611-thumbnail.jpg?width=640&height=640&fit=bounds)
























![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




