Downloaded 186 times



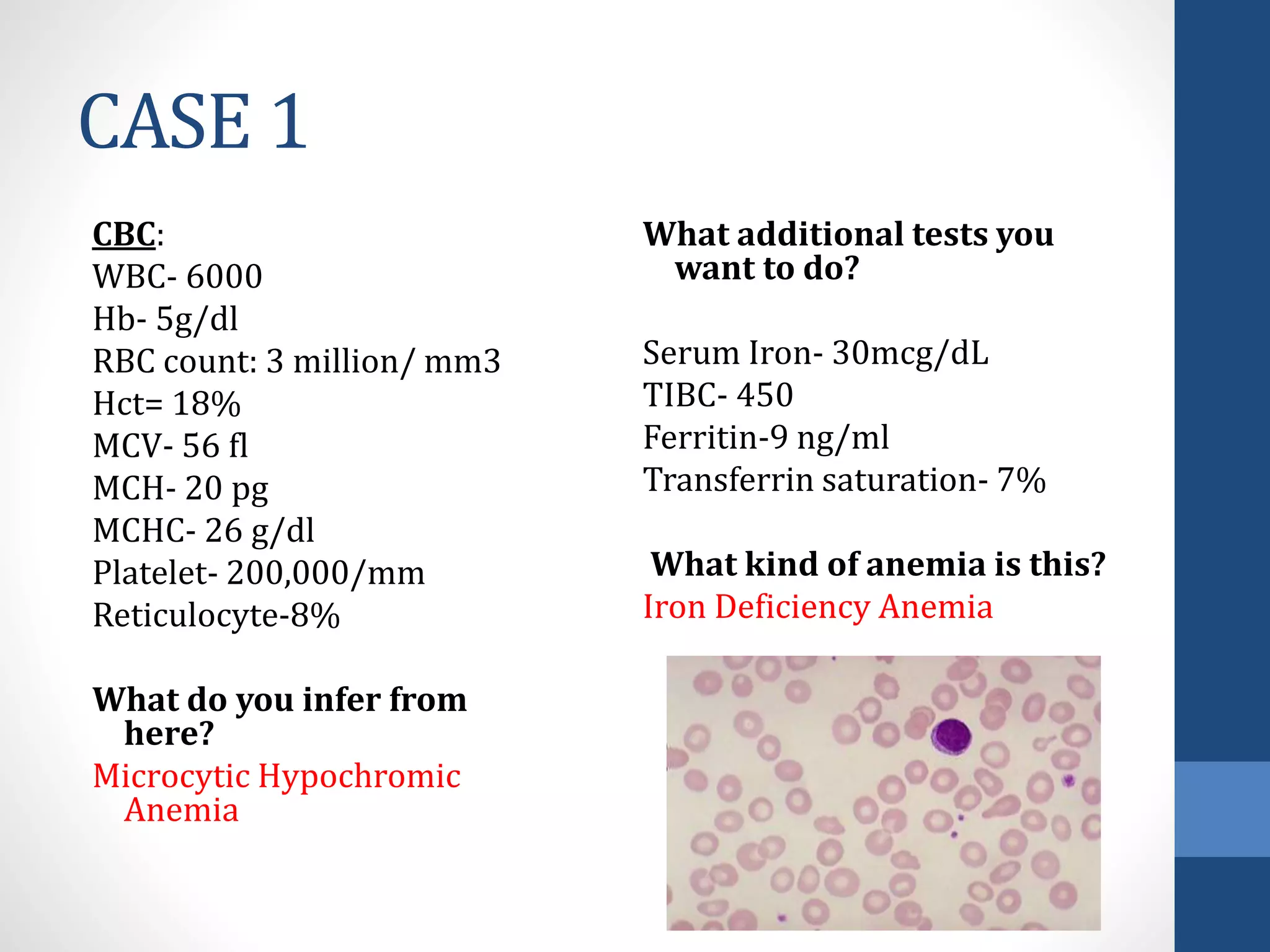




































This document provides an outline and overview of different types of anemia, including how to approach a patient with anemia and classify different types. It also includes 6 case studies of patients presenting with anemia. The cases demonstrate how to interpret lab results to make a diagnosis of anemia type, such as iron deficiency anemia, beta-thalassemia, aplastic anemia, sickle cell anemia, folate deficiency anemia, and viral hepatitis-related anemia. The document discusses diagnostic testing and management approaches for each case.



































































